
Rhabdomyolysis, in its simplest definition, is a condition where the intracellular components of skeletal muscle cells are released and enter the bloodstream. An article published in Clinical Chemistry and Laboratory Medicine in March of 2010 defines it as “…..the rapid break-down of striated muscle.” (Cervellin, Comelli, & Lippi, 2010) To better understand rhabdomyolysis, my project will cover the different energy molecules in the cell and their use in anaerobic and aerobic exercise. Rhabdomyolysis can cause some real damage to our other systems, but how exactly does this happen? There are two ways that the breakdown of striated muscle cells can occur: direct and indirect.
The direct method is caused by physical trauma to the muscle. This can be caused by physical impact trauma, such as a fall or accident or impingement under extreme load for an extended time. Road accidents are the most common type of direct trauma that leads to rhabdomyolysis. (Cervellin, Comelli, & Lippi, 2010) The indirect method, exertional rhabdomyolysis, is caused by intense physical exercise or participation in an exercise beyond an accustomed level of intensity. (Luetmer, et al., 2020) Muscle action requires adenosine triphosphate (ATP) as energy to facilitate muscle contraction and plays a vital role in maintaining ionic balance inside the cell via the protein pumps in the cell membrane. These pumps generate transmembrane transport and facilitate action potentials by pumping sodium and potassium against their concentration gradients to maintain intracellular negative charge. (Betts, et al., 2022) Keeping a higher concentration of sodium extracellular and potassium intracellular. In addition to creating this gradient, ATP is the only source of energy to fuel muscle contractions and is also required to turn that contraction off. To generate ATP the body uses aerobic and anaerobic pathways to convert glucose into ATP.
The aerobic pathway generates ATP in the presence of oxygen, making it the body’s primary energy system during prolonged, moderate-intensity activities. This process occurs in the mitochondria of cells and involves glycolysis, the Krebs cycle, and the electron transport chain (ETC). Initially, glucose is broken down into pyruvate during glycolysis, yielding a small amount of ATP and NADH. Pyruvate is then transported into the mitochondria and enters the Krebs cycle. This cycle generates high-energy electron carriers (NADH and FADH2), which deliver electrons to the ETC (Betts, et al., 2022). In the ETC, oxygen acts as the final electron acceptor, producing a significant amount of ATP—approximately 36-38 molecules per glucose molecule. The aerobic system is efficient but slower than anaerobic systems due to its dependence on oxygen delivery and availability.
The anaerobic pathway generates ATP in the absence of oxygen, making it the suitable energy system during short, high-intensity activities. Anaerobic glycolysis is the main pathway involved, where glucose is rapidly broken down into pyruvate in the cytoplasm, producing a small yield of ATP—approximately two molecules per glucose, ~5% as much as that generated by the aerobic pathway. Without sufficient oxygen, pyruvate is converted into lactate, which can accumulate and lead to muscle fatigue (Betts, et al., 2022). The anaerobic pathway is faster than the aerobic system, providing energy quickly to meet immediate demands. Still, it is less efficient and cannot sustain prolonged activity due to limited glucose stores and the buildup of metabolic byproducts. The body also employs direct phosphorylation of adenosine diphosphate by creatine kinase, a form of anaerobic metabolism that utilizes creatine phosphate to regenerate ATP almost instantaneously. Still, this system is only effective for bursts of energy lasting about 10 seconds (Betts, et al., 2022).
During intense physical activity, the body, through anaerobic and aerobic processes, may not be able to keep up with the ATP necessary to do the physical work and power the pumps essential for cellular homeostasis. This is caused by the availability of oxygen to the system to support aerobic and anaerobic pathways used depending on the workout’s intensity level and whether that pathway can support it. Anaerobic pathways are faster but get less bank for your buck, but there may not be enough oxygen to support the aerobic pathway. When there is insufficient ATP to support these protein pumps and efficient muscle contractions, several things happen. The concentration of ions begins to naturally move down their gradient, creating an influx of sodium and calcium intracellular and potassium extracellular. The increase in calcium leads to prolonged muscle contraction and further depletes ATP (Luetmer, et al., 2020). The increase in sodium draws water into the cell via osmosis, causing edema and damaging the integrity of the cell wall.
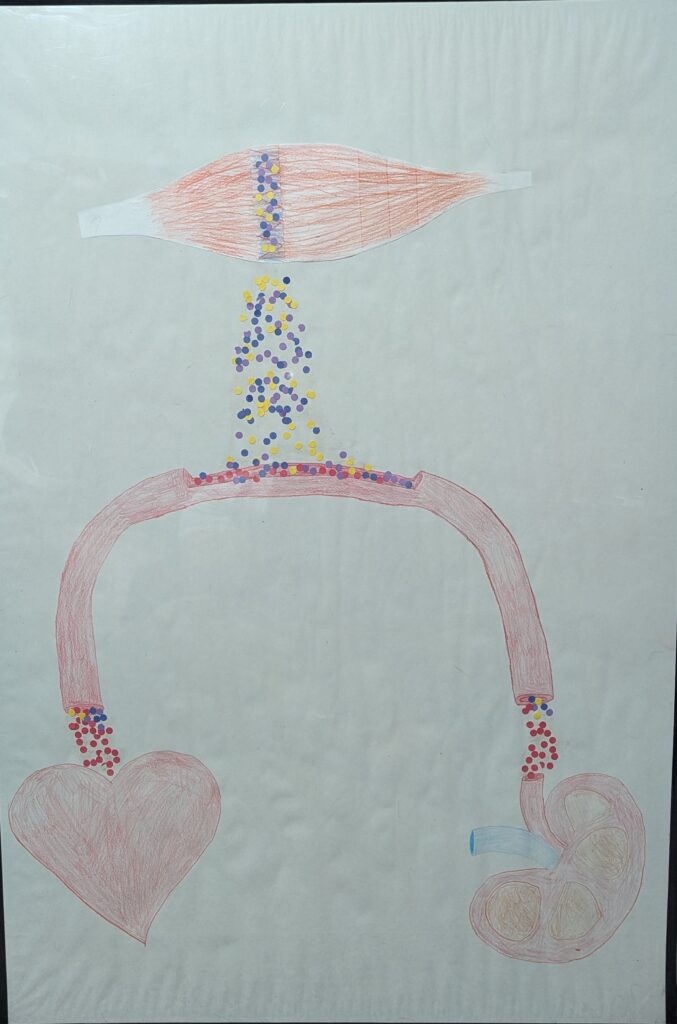
Whether directly or indirectly, damage to the muscle fiber’s integrity leads to the release of muscle cell components, potassium, phosphates, myoglobin, creatine kinase (CK), and urates into the bloodstream and can cause many health complications. (Cervellin, Comelli, & Lippi, 2010) This release into the bloodstream can cause severe muscle pain, weakness, and swelling at the location of the affected muscle. Acute renal failure due to increased myoglobin in the blood overtaxing the kidneys, which may be indicated in color variations of urine, ranging from pink to black. (Cervellin, Comelli, & Lippi, 2010) Other symptoms are metabolic acidosis, electrolyte abnormalities, and cardiac arrhythmias caused by increased blood potassium levels. (Luetmer, et al., 2020). One of the methods used to detect rhabdomyolysis is an elevated state of creatine kinase. (Luetmer, et al., 2020) In cases of direct damage, the elevation of CK might be a key indicator, but this can be more challenging in indirect induction, because a certain amount of CK is created during regular exercise. Because of this, the accepted standard for CK as an indicator of rhabdomyolysis is five times the upper limit of normal as the cut-off for diagnosis. (Luetmer, et al., 2020)
References
Betts, J. G., Young, K. A., Wise, J. A., Johnson, E., Poe, B., Kruse, D. H., . . . DeSaix, P. (2022). Anatomy and Physiology 2e. Houston, Texas: OpenStax. Retrieved from https://openstax.org/books/anatomy-and-physiology-2e
Cervellin, G., Comelli, I., & Lippi, G. (2010). Rhabdomyolysis: historical background, clinical, diagnostic. Clinical Chemistry and Laboratory Medicine, 749-756. doi:0.1515/CCLM.2010.151
Luetmer, M. T., Boettcher, B. J., Franco, J. M., Reisner, J. H., Cheville, A. L., & Finnoff, J. T. (2020). Exertional Rhabdomyolysis: A Retrospective Population-based Study. Medicine & Science in Sports & Exercise, 52(3), 608-615. doi:10.1249
