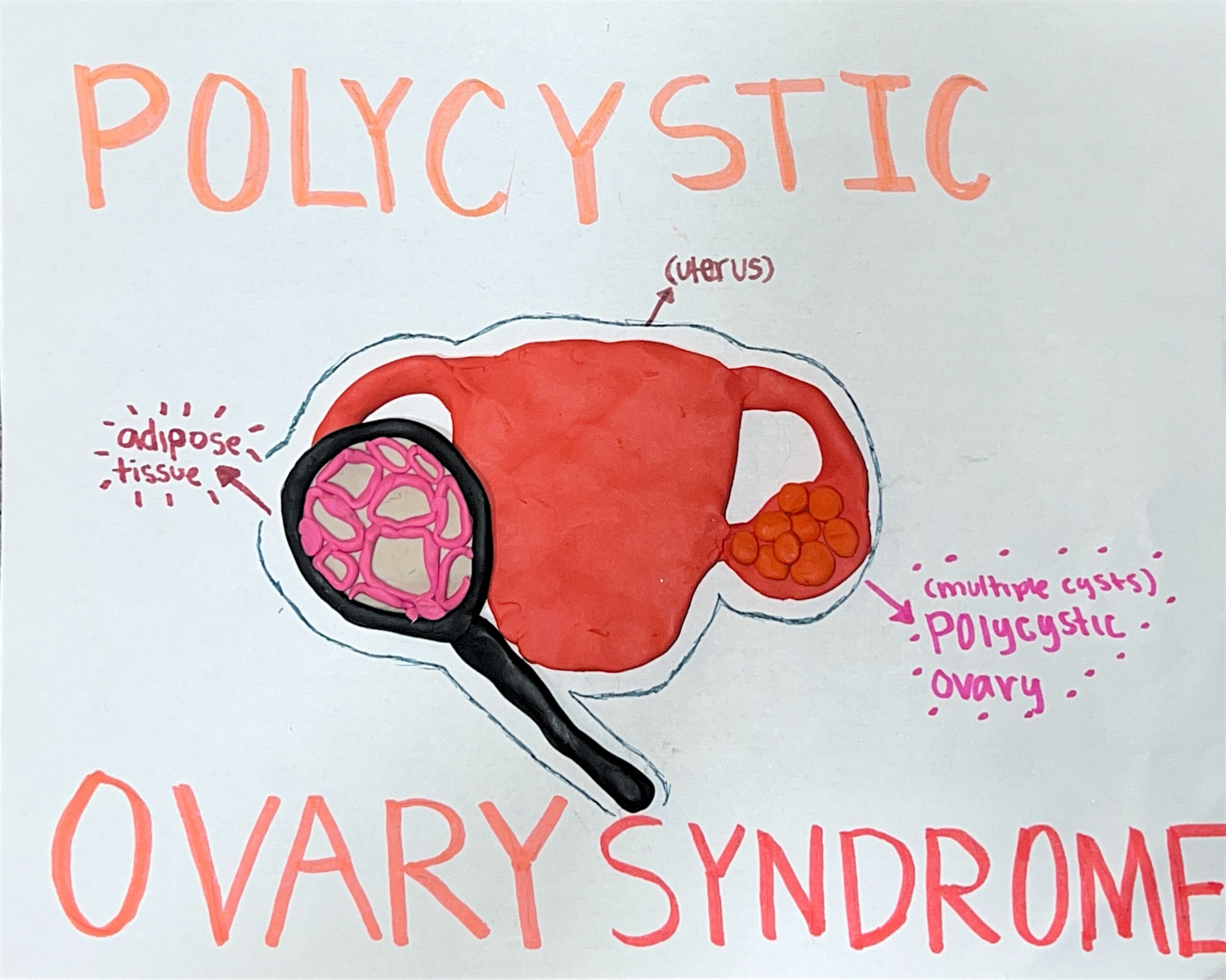
My STEAM project covers Polycystic Ovary Syndrome (PCOS). More specifically, it will be covering how the body responds to adipose tissue in the ovaries due to PCOS. My project covers the objective “Describe in depth each type of epithelial and connective tissue. Be able to describe their function and location.” The medium that I am using with my project is clay art. I will be using reference websites, and I will also be using personal experience describing what PCOS is.
To understand how adipose tissue in the ovaries affects someone with PCOS, we need to understand what that tissue is and what PCOS is. Adipose tissue is a connective tissue, all connective tissues have the same embryonic origin, they have varying degrees of vascularity, and all cells are suspended/embedded in an extracellular matrix (ECM). Under connective tissues there are three branches, adipose tissue is categorized in the connective tissue proper branch. After that, there are loose or dense connective tissue, and adipose tissue is categorized as loose connective tissue. When we look at the clay art that I made and look at the adipose tissue, we can see it is very spacious, and there is a background color representing an ECM. The characteristics of adipose tissue are that they are richly vascularized, they have a scanty matrix, and they are similar to areolar tissue, but they have a greater nutrient storage. They function in shock absorption, insulation, and energy storage. Their primary location is in the abdomen and breasts, around the kidneys and eyeballs, and under skin in the subcutaneous tissue. Their cells are also called adipocytes.
Polycystic Ovary syndrome is a common reproductive syndrome. According to the Frontiers in Endocrinology (2022), “PCOS is a common metabolic and reproductive syndrome with heterogenous clinical presentations (‘syndromes’) that have no simple, single diagnostic or clinical management pathway.” This issue makes it very common for many people to go undiagnosed, or to get a wrong diagnosis. PCOS is diagnosed with the Rotterdam criteria, which says that to get diagnosed with PCOS one must have two of three criteria: oligo-ovulation, hyperandrogenism and polycystic ovaries. Some side effects of PCOS are type 2 diabetes, cardiovascular disease, insulin resistance, obesity, infertility, pregnancy complications, sleep disturbances, hypothyroidism, decreased mental health, non-alcoholic fatty liver disease (NAFLD), extra body hair, acne, high testosterone levels, and so much more! We still don’t know what causes PCOS or any cures, but we know how we can manage our symptoms and lower them.
When I started getting PCOS symptoms, I was in middle school, so 13 or 14, and when I went to the doctors, the lady who was my nurse told me, “What has a tail and four legs?” and I said a dog. She said, “That’s true, or it could be a zebra, but most likely it would be a dog. Your hormones are still leveling out so you don’t have much to worry about.” I was sent home told to eat healthier and start going to the gym. This response is one example of not being diagnosed properly. I had to live with the symptoms until I went to a womens healthcare facility and got properly diagnosed.
So how does adipose tissue play a role in PCOS and the ovaries? Well, we can develop adipose tissue dysfunction. According to The Journal of Clinical Endocrinology & Metabolism (2023), “In addition to adipocytes, AT is also composed of macrophages and other stromal cells, which play an important role in inflammation and cytokine release. Therefore, when AT becomes dysfunctional, a cascade of metabolic derangements is triggered, with systemic repercussions (24). The exact mechanisms that initiate AT dysfunction have not been well established. Indeed, these mechanisms may be considerably different depending on whether AT dysfunction is being promoted by genetic, epigenetic, and/or environmental factors.” Some of the symptoms people can get from adipose tissue dysfunction are obesity, insulin resistance, metabolic syndrome features, increased risk of diabetes, and infertility. It can also be characterized by hypertrophic adipocytes, impaired lipolysis, impaired insulin action, and altered expressions and secretion of adipokines. “Aside from the well-established role of insulin resistance and hyperinsulinism as facilitating factors for androgen excess [14], molecules secreted by adipose tissue might also influence adrenal and ovarian function, and adipose tissue itself directly intervenes in the metabolism of steroid hormones.” (Escobar-Morreale et al., 2007)
In conclusion, adipose tissue contributes to PCOS and has the effects of obesity, insulin resistance, metabolic syndrome features, increased risk of diabetes, infertility, increased risks for cardiovascular diseases, elevated androgens, irregular menstrual cycles, and inflammation. From what I have read, it seems as if it elevates symptoms of PCOS.
CITATIONS: Emanuel, R. H. K., Roberts, J., Docherty, P. D., Lunt, H., Campbell, R. E., & Möller, K. (2022, November 15). A review of the hormones involved in the endocrine dysfunctions of polycystic ovary syndrome and their interactions. Frontiers in endocrinology. https://pmc.ncbi.nlm.nih.gov/articles/PMC9705998/
Bril, F., Ezeh, U., Amiri, M., Hatoum, S., Pace, L., Chen, Y.-H., Bertrand, F., Gower, B., & Azziz, R. (2023, December 21). Adipose tissue dysfunction in polycystic ovary syndrome. The Journal of clinical endocrinology and metabolism. https://pmc.ncbi.nlm.nih.gov/articles/PMC10735305/
Wickenheisser, J. K., Poretsky, L., Goumenou, A. G., DeUgarte, C. M., Nagamani, M., Franks, S., Gonzalez, F., Fenkci, V., Norman, R. J., Sabuncu, T., Carmina, E., Diamanti-Kandarakis, E., Asunción, M., Azziz, R., Zawadzki, J. K., Escobar-Morreale, H. F., Gambineri, A., Dunaif, A., DeClue, T. J., … Taylor, S. I. (2007, August 10). Abdominal adiposity and the polycystic ovary syndrome. Trends in Endocrinology & Metabolism. https://www.sciencedirect.com/science/article/pii/S1043276007001129#:~:text=Abdominal%20adiposity%2C%20overweightness%20and%20obesity,and%2C%20possibly%2C%20adrenal%20hyperandrogenism.