
The nervous system consists of both the central nervous system (CNS) and the peripheral nervous system (PNS) (Ohana, et al., 2014). The CNS includes the brain, spinal cord, and retina. (Ohana, et al., 2014). The PNS includes all other nervous structures. Such structures include nerves, ganglion, various receptors, and motor nerve endings (Ohana, et al., 2014).
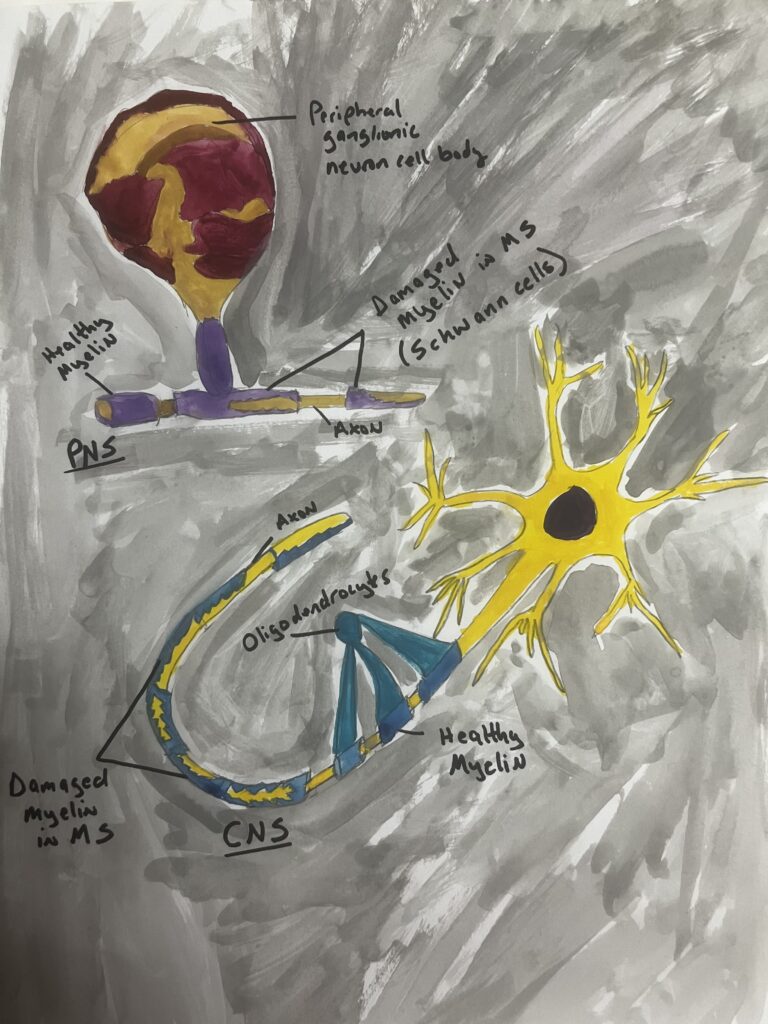
The purpose of the PNS is to facilitate CNS commands to organs and return internal and external sensory information (Ohana, et al., 2014). The peripheral nerve is a rope-shaped concentric structure (Ohana, et al., 2014). The peripheral nerve consists of an axon, which is long and extends from the neuronal cell body that is specialized to transport the nerve impulse (Ohana, et al., 2014). The nerve is sheathed in a support cell called the Schwann cell, which has two different types of fibers: unmyelinated and myelinated (Ohana, et al., 2014). Unmyelinated fibers are surrounded by a single layer of Schwann cytoplasm and conduct nerve impulses slowly (Ohana, et al., 2014). Such fibers tend to conduct sensory (pain) and vegetative functions (Ohana, et al., 2014). In contrast, myelinated fibers are surrounded by multiple layers of Schwann cytoplasm to form a myelin sheath (Ohana, et al., 2014). Myelinated fibers are involved in rapid responsive conduction for somatic motor fibers and sensory fibers (Ohana, et al., 2014).
Multiple sclerosis (MS) is a complex multifactorial neuroinflammatory and autoimmune disease that is associated with damage to axonal myelin sheaths and neuronal degeneration. (Macchi, et al., 2015). The disease is considered the most common disabling neurological disease in young adults after traumatic brain injury. (Macchi, et al., 2015).
The characteristic event in MS is oligodendrocyte loss (via cell apoptosis) accompanied by axonal damage, blood-brain barrier (BBB) leakage, and inflammation and infiltration of immune cells (Macchi, et al., 2015). Oligodendrocytes are a type of glial cell in the CNS that produce myelin sheaths around axons. (Betts, et al., 2022). Further, dysfunction of the BBB causes lymphocytes to invade the CNS, causing activation of autoimmune T cells, microglia, and macrophages, all of which results in a cascade of abnormal immune responses. (Macchi, et al., 2015). Additionally, as the disease destroys the myelin surrounding the axons, scarring in the white matter of CNS (brain and spinal cord) becomes more obvious. (Betts, et al. 2022). While the etiology of MS remains unclear, certain drugs that both prevent immune cells from entering the CNS and deplete certain lymphocytes have been highly effective in treating MS. (Adamec, et al., 2021).
While the PNS is not officially considered in the diagnostic criteria for MS, there is increasing evidence of peripheral nerve involvement (Foesleitner, et al., 2023). For example, high resolution MR neurography (MRN) of MS patients demonstrated structural changes in peripheral nerves and inflammatory PNS involvement based on markers evidencing demyelinating processes in the Schwann cells (Foesleitner, et al., 2023). Another study found that MS-patients had a lower sweating response when compared to healthy controls due to abnormal sweating functions caused by preganglionic lesions affecting the autonomic nervous system (Adamec, et al., 2021). Further, MRI imaging has also shown that PNS lesions in MS are likely to be caused by immunologic reactions and destructions of molecules within the myelin sheath. (Adamec, et al., 2021).
Accordingly, there is evidence of both CNS and PNS involvement in MS based on imaging studies, somatic and autonomic effects of the disease, and the efficacy of drug therapies that attempt to maintain the blood-brain barrier and reduce the autoimmune response. Because both the CNS and PNS contain myelin insulated axons that facilitate the transmission of electrical signals, demyelination can occur in both parts of the nervous system and contribute to MS. (Betts, et al. 2022).
Literature Cited
Adamec I, Skoric MK, Habek M. (2021). Peripheral nervous system in multiple sclerosis – understanding the involvement via autonomic nervous system. Neurological Sciences. 42:2731-2736. https://doi.org/10.1007/s10072-021-05309-9.
Betts, J. G., Young, K. A., Wise, J. A., Johnson, E., et al. (2022). Anatomy and Physiology 2e. OpenStax.
Foesleitner O, Volker S, Hayes J, Weiler, et al. (2023). Microstructural changes of peripheral nerves in early multiple sclerosis: A prospective magnetic resonance neurography study. European Journal of Neurology. doi:10.1111/ene.16126.
Macchi B, Marino-Merlo F, Nocentini U, et al. (2015). Role of inflammation and apoptosis in multiple sclerosis: Comparative analysis between the periphery and the central nervous system. Journal of Neuroimmunology. 287:80-87.
Ohana M, Moser T, Moussaoui A, Kremer S, et al. (2014). Current and future imaging of the peripheral nervous system. Diagnostic and Interventional Imaging. 95:17-26.
The central nervous system includes the brain, spinal cord, and retina The peripheral nervous system includes all other nervous structures. These two systems are a part of the nervous system and include nerves, ganglion, various receptors, and motor nerve endings. The peripheral nerve is a rope-shaped concentric structure that facilitates the central system to command organs and return the sensory information from external and internal. The peripheral nerve consists of an axon that extends from the neuronal cell body specializing in transport of the nerve which is composed of two different types of fibers unmyelinated conduct nerve impulses slowly like pain sensory and vegetative functions and myelinated is a rapid response of conduction for somatic motor fibers and sensory fibers and together they make up a Schwann cell. Multiple sclerosis also known as MS is a common neurological disease that is a complex multifactorial neuroinflammatory and autoimmune disease that has damage to axonal myelin sheaths and neuronal degeneration. Symptoms involving MS oligodendrocyte loss, axonal damage, blood-brain barrier leakage, and inflammation and infiltration of immune cells. Certain drugs can prevent immune cells from entering the CNS and deplete certain lymphocytes and are effective in treating multiple sclerosis. There’s also increasing evidence of peripheral nerve involvement, even though it’s not officially considered diagnostic criteria. A study was conducted and results showed that MS-patients had a lower sweating response when compared to healthy control groups. That is because of the abnormal sweating functions caused by preganglionic lesions which in return affect the autonomic nervous system. Finding evidence of both CNS and PNS involvement was found in imaging studies, and drug therapies were used to try maintaining BBBs and reduce one’s autoimmune response.