

Objective: 44. Describe how respiration is regulated.
The function of the lungs is to facilitate the gas exchange of oxygen and carbon dioxide to provide your tissues with oxygen but also get rid of the waste products like carbon dioxide. But what if that function is hindered by conditions that physically restrict the lung from moving oxygen in and carbon dioxide out? There are three conditions that do that very thing. There is the pneumothorax, hemothorax, and hemopneumothorax. Each condition has both different and similar causes but all are the same in physically restricting the expansion of the lungs.
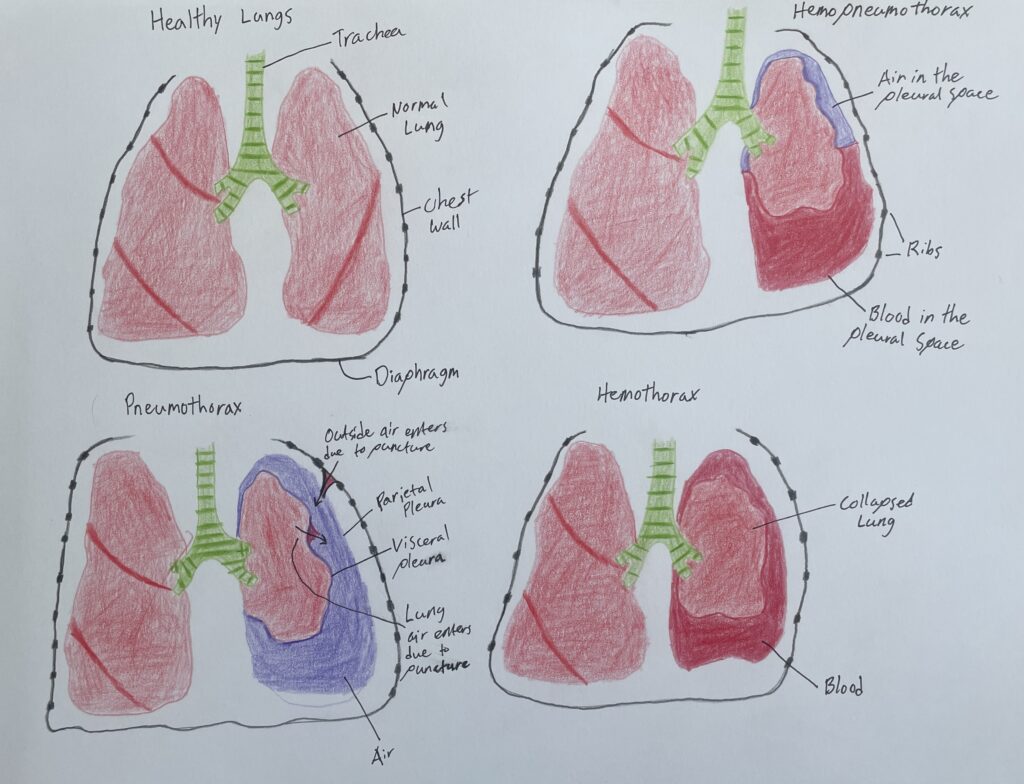
The pneumothorax is a collection of air outside of the lung in the pleural cavity. The air accumulation can apply pressure on the lung making it extremely difficult to expand which can eventually lead to a collapsed lung. A pneumothorax can be caused by either atraumatic or traumatic events. Atraumatic pneumothorax is known as a spontaneous pneumothorax which is caused by the rupture of a bleb on the lungs. Traumatic pneumothorax is caused by blunt or penetrating trauma. To confirm your suspicion for a pneumothorax a CT, X-ray, or ultrasound should be performed to image any broken bone or air in the pleural space. To treat any pneumothorax that shows signs of instability you can administer a needle chest decompression (NCD) as a temporary solution. For this you will insert a 12 or 14 gauge needle 4.5 cm in length with an angiocatheter. This recently changed in the military medicine world where a 10 gauge needle with at least a 3.25 inch long angiocatheter is used. This needle is inserted perpendicular to the chest along the midclavicular line above the 3rd rib in the 2nd intercostal space. Alternatively it can be inserted anterior to the midaxillary line in the 5th intercostal space just above the 6th rib. You can do multiple NCDs if instability continues to attempt to release the trapped air. The gold standard treatment is a thoracostomy where a chest tube is inserted in the 5th intercostal about the 6th rib just anterior to the midaxillary line. The size of the tube is dependent on the size of the patient or if there is a hemothorax present. For an open ‘sucking’ chest wound, only caused by penetrating trauma, a chest seal with at least 3 sealable sides has to be applied on top of the wound. Although if instability occurs with a chest seal applied you should attempt to peel back the seal to attempt to ‘burp’ the wound before performing an NCD. The thing to remember is that the definitive treatment for pneumothorax is a thoracostomy to help get the air out of the pleural space, allow for life-supporting breathing, and allow for the damaged tissue to heal.
A hemothorax refers to the collection of blood outside the lung in the pleural cavity. The collection of blood can compress the lungs restricting the expansion of the lungs. This condition only occurs from the rupture of blood vessels of the lung or chest wall either from trauma or other physiological reasons. You can confirm your suspicions with an X-ray or CT scan to show the source of bleeding or any broken bones. The treatment for this is a chest tube to drain the blood out although if you are not able to have this done now you could result in an NCD as it is better than nothing. Surgery should also be considered to repair the source of any major bleeding to stop the condition from worsening. Of course, blood transfusions should be considered as the body is losing blood so volume may need to be replaced.
The hemopneumothorax is a combination of a pneumothorax and a hemothorax but very rarely does a hemothorax occur without a pneumothorax. This condition usually occurs as a result of a gunshot wound, broken rib, stabbing, or other traumatic events. The treatments for this condition are almost exactly the same as the pneumothorax although considerations should be taken. For example, a larger NCD needle should be used if available but the patient should be evaluated more in case blood clots start to clog the needle catheter which makes it ineffective so additional NCDs may need to be placed. You should also use a larger chest tube to avoid clogging and you should monitor the flow of blood out of the tube to identify any blood clots stopping the draining of the pleural cavity. Surgery should also be considered to repair the source of any major bleeding to stop the condition from worsening. The overall goal for a thoracotomy is to drain the blood from the pleural space faster than it bleeds into the cavity but blood transfusion should always be considered to replace the lost blood.
The function of the lungs relies on the expansion and deflation of them to move in oxygen then move out carbon dioxide. Without this function the body could not survive from lack of oxygen. There can be physical hindrances that stop this function from conditions like pneumothorax, hemothorax, and hemopneumothorax. These conditions will fill the space between the visceral and parietal pleura which puts pressure on the lungs keeping them from expanding. If intervention is not made it will become impossible for a person to breathe.
References
Cafasso, J. (2018, September 18). Hemopneumothorax: Treatment, symptoms, and causes. Healthline. Retrieved April 20, 2023, from https://www.healthline.com/health/hemopneumothorax
Catherine, M. K., & Bracken, B. (2023, February 15). National Center for Biotechnology Information. Pneumothorax. Retrieved April 21, 2023, from https://www.ncbi.nlm.nih.gov/books/NBK441885/
Jewell, T. (2017, August 28). Hemothorax: Definition, symptoms, and treatment. Healthline. Retrieved April 20, 2023, from https://www.healthline.com/health/hemothorax#diagnosis