
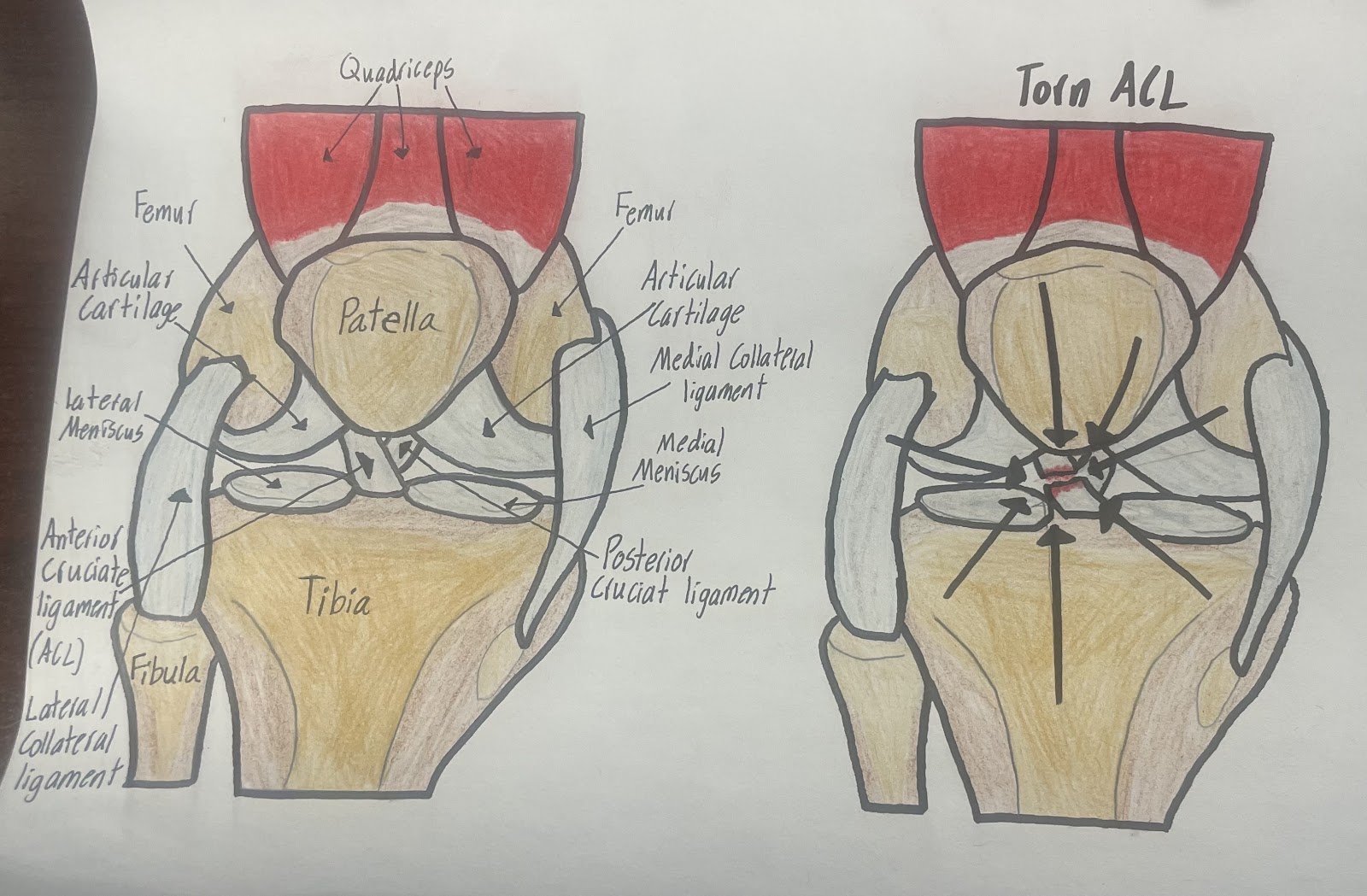
The objective I am covering for my STEAM project is knowing the structure of the knee joint. We learned about the knee joint during unit 4. We learned that the knee is the largest and most complex joint. The knee is where the femur and tibia meet. The patella (kneecap) is anterior to the femur and tibia. We further learned about the anterior cruciate ligament, ACL, and how to prevent the tibia from sliding forward and stopping hyperextension. The knee is made of dense regular connective tissue, which means it’s stable in one direction. Blows to the side or twisting forces can cause a tear in the ACL. A couple of fascinating lecture videos on ACL reconstruction surgery show how the surgery is performed. For my project, I researched ACL reconstruction surgery in depth. I chose this topic because I completely tore my ACL, and partially tore my medial collateral ligament and meniscus while I was playing basketball. Due to my injury I needed ACL reconstruction surgery. My ACL was constructed using my patellar tendon. For my art piece, I drew two structures of the knee, one with a non-injured knee and the other with a torn ACL.
There are two tests a doctor can use to check if the ACL is partially or completely torn. The first test is the Lachman test, in which the doctor tries pulling the shin away from the thigh. If the bones do not move or have minimal movement, the ACL is still intact but torn. The second test is done with the patient on their back and the doctor lifts the leg and puts rotational pressure on the knee. If there is no shift in the bone, it is not torn. People who have a partial ACL tear may or may not need surgery. Partial tears may have the ability to heal on their own, but complete tears cannot. Surgery for a complete tear of the ACL is usually recommended for full strength but not always. If someone is inactive or does not exercise there are nonsurgical treatments. These treatments are not suggested for physically active individuals. Contact exercises with a completely torn ACL are not recommended because further injury is a risk such as tearing the meniscus.
There are lots of decisions to be made my the doctor and patient before for reconstruction surgery of the ACL. The ACL has two parts termed “bundles”: the anteromedial (AM) and the posterolateral (PL) bundles. These bundles work together and stabilize the knee. There is a double bundle and single bundle reconstruction surgery for the ACL. Double bundle reconstruction focuses on restoring structure and knee movement, but the surgery is much more complex and may cause more bone loss. This surgery may be better for those who have lots of instability or for someone who needs another surgery. The single bundle surgery is the most common surgery for the ACL. This method focuses on only one part of the knee, the AM. This surgery prevents the knee from moving too far forward and backward but sometimes doesn’t entirely fix the rotation and twisting movements.
The surgery has three entry points: the AM portal, the anterolateral (AL) portal, and the accessory medial portal (AMP). The entry point used during surgery depends on the tear and the doctor’s expertise. There are lots of different graft (tissue) options to choose from to replace the ACL. The factors for determining what to choose are age, gender, physical activity level, the thickness of tendons, and the original ACL and bone structure. The grafts used are the patellar tendon, quadriceps tendon, hamstring tendon, or donor. The most popular grafts are the hamstring and patellar tendon.
The doctors will make an incision based on the graft used. The graft will is removed as it is used has the new ACL, and the incision will be stitched. The graft is then sized correctly for the patient. The doctors use an arthroscopy through the AL portal. An arthroscopy is a tube attached to a specialized camera that allows doctors to see the inside of joints. It is shown on large screens, allowing the doctor to see inside. They look for the ACL tear and for any other injuries that might have happened. The torn ACL is then removed. To correctly place the tunnels, doctors will look at the leftover parts of the old ACL and ridges in the knee. The tunnels are made with the correct distance between the AM and PL bundles for a single bundle reconstruction. For a double bundle, tunnels are made where the AM and PL bundles connect. A fastening suture is attached to the tunnel to help pull the graft through.
The new ACL is then held into place by a fixation device on the thighbone. The fixation device is used on the graft to be secure and properly healed. These devices give strength to the graft. The devices are picked based on the type of graft and bone quality. The knee is bent and straightened constantly because the new ACL usually stretches and can loosen a bit. The fixation device pulls the graft tightly and attaches to the shinbone. The knee bends at 20 degrees during this step. The doctor will then examine the knee and ensure no problems have arisen.
The knee is the most complex and the largest joint in the body, where the femur meets the tibia. Within this joint, the anterior cruciate ligament, ACL, prevents the tibia from sliding forward, thus preventing hyperextension. The ACL is made of dense regular tissue, which is only stable in one direction, and is made up of the anteromedial and posterolateral bundles that stabilize the knee. Twisting forces, or blows to the side of the knee can cause the ACL to tear. Doctors can use two tests to check if a damaged ACL is either partially or completely torn. Those with a partial tear may not need surgery, and may heal on their own, but a complete tear requires surgery. ACL reconstruction surgery can consist of double or single bundle reconstruction. There are three entry points for reconstruction: AM, AL, or AMP portals, depending on the tear and what graft is used. There are many different graft options to replace the ACL, the most common being the hamstring or patellar tendon. Many factors determine what graft option is used is based on age, sex, physical activity, ect. The surgery involves the removal of the graft, sizing the graft, removal of the torn ACL, and replacing it with the graft. A fixation device is then placed on the thigh bone to ensure security and healing of the new ACL.