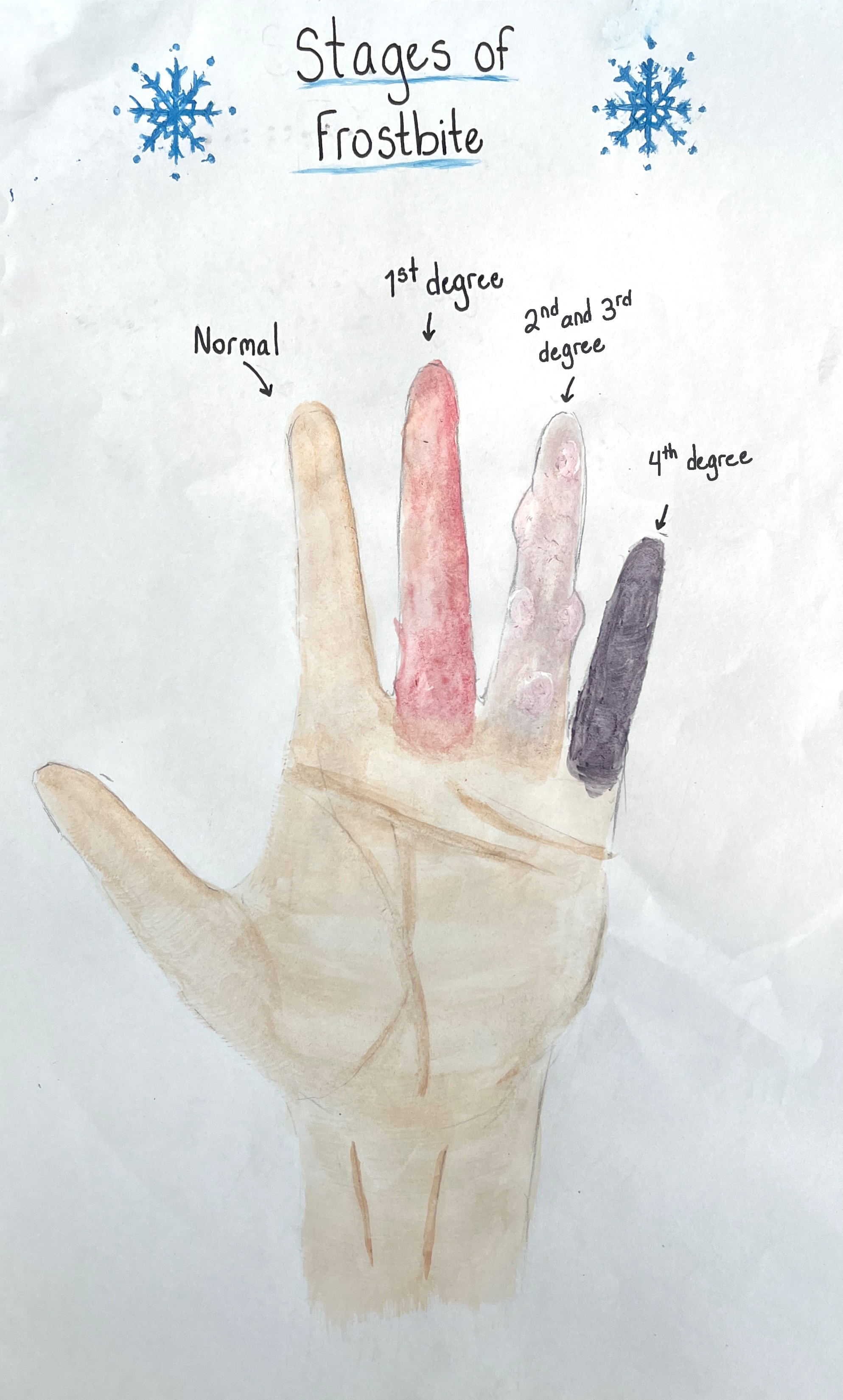
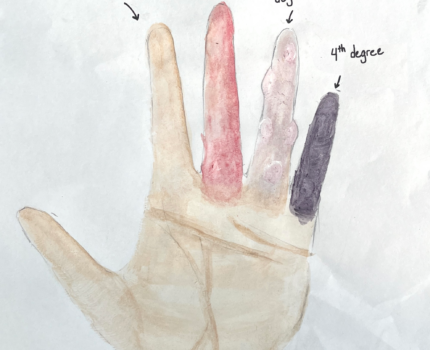
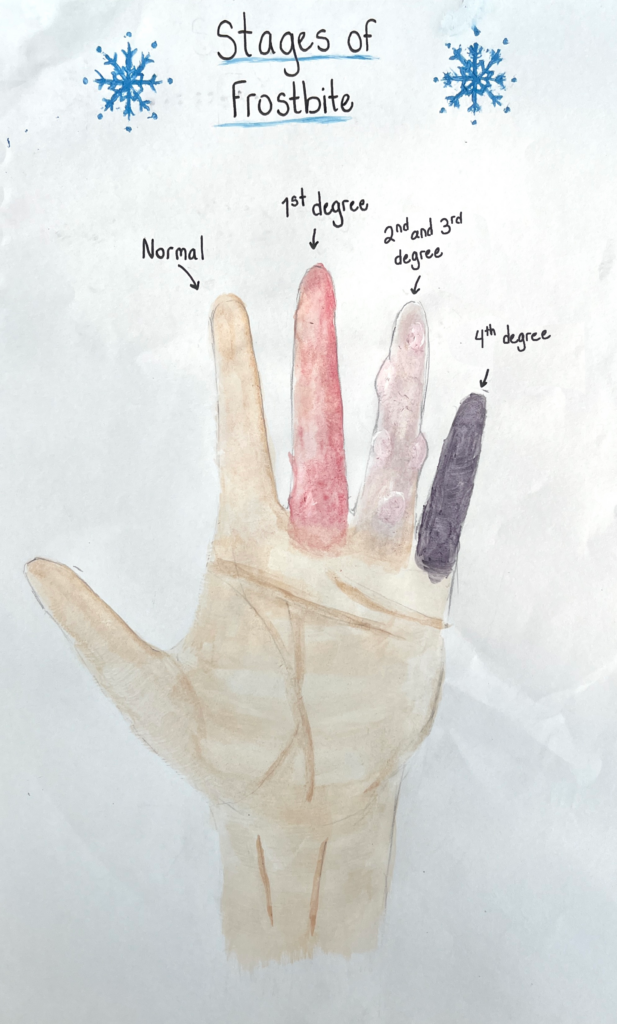
The course objective my project relates to is the functions of the integumentary, specifically how it leads to frostbite and what frostbite looks like. Frostbite may begin as frostnip and becomes frostbite when one’s tissue freezes (Alexander et. al 2024, p.3). The extent of damage to the tissue depends on how long the area is exposed to the cold temperatures. Frostbite damage is typically classified into 4 degrees, which can be seen in my project (Mclntosh et. al 2024, p.184). However, it is difficult to tell the extent of the damage when the tissue is still frozen and without imaging (Mclntosh et. al 2024, p.184). This is why there are different methods of determining the degree of frostbite. For example, some may determine the degree of frostbite by appearance of the skin, or by how far the frostbite extends across the skin, or the depth of tissue damage. My project visually represents what the different degrees of frostbite look like on the skin. First degree frostbite can be identified, after thawing, by the skin color, the skin will appear red. Tissue damage in first degree frostbite is minimal and considered superficial meaning it has only affected the surface of the skin (Mclntosh et. al 2024, p.184). Second and third degree frostbite look similar, which is why they are the same in my project. In second and third degree frostbite the skin appears white, possibly gray and blistered. The blisters will also be white and are the lumps seen on the ring finger of my project. However, second degree frostbite has only superficial tissue damage, while third degree frostbite has deep tissue damage that extends to the reticular layer of the dermis (Mclntosh et. al 2024, p.184). Lastly, fourth degree frostbite has deep tissue damage extending all the way to the muscle and bone (Mclntosh et. al 2024, p.184). That is why fourth degree frostbite typically results in amputation, because the necrosis has spread to muscle, bone, tendons, and blood vessels and they can no longer heal. In fourth degree frostbite the skin after thawed and possibly after a few days will be a dark purple and black color. I specified after you thaw the tissue in all of the examples because before you thaw the tissue, frostbite, of any degree, will usually appear white. This is because when our body temperature drops our bodies attempt to maintain homeostasis by keeping our internal organs warm. To do this the arterioles constrict forcing the blood to circulate below the surface of the skin, therefore minimizing heat loss and keeping our core warm (Betts et. al 2022 p.179). However when it is too cold outside this causes the skin to freeze because heat from the blood is not circulating close to the surface and this is also why our skin appears white when we are cold and when we have frostbite (Betts et. al 2022 p.179). In my project the frostbite is displayed as affecting the whole finger, however it is possible and not unusual for frostbite to only affect the distal end, it may not affect all the way to the proximal end, it depends on how much of the skin is exposed. This is why an important part of preventing frostbite is covering the skin. Minimizing the amount of tissue exposed to outside air helps prevent frostbite because it keeps the body dry and keeps off the wind, helping the skin stay warm (Mclntosh et. al 2024, p.185). It is recommended that when you first realize you have frostbite you quickly rewarm or thaw out the tissue (Alexander et. al 2024, pp.5-6). This is to see the extent of the damage and by warming the skin blood flow will return, as long as there is not too much damage.
ABSTRACT
Jazz’s STEAM project explores the impact of frostbite on the integumentary system, focusing on its progression from frostnip to severe frostbite. The image represents the differing degrees of frostbite, utilizing classification into four degrees based on the extent and depth of tissue damage. Frostbite begins as frostnip, with initial symptoms being minimal and superficial. As exposure to cold increases, the tissue can freeze, leading to more severe damage classified into four degrees.
In first-degree frostbite, which affects only the skin’s surface, the damage is minimal and results in red discoloration after thawing. Second and third-degree frostbite present similarly, with white or grayish skin and blisters, though the latter involves deeper tissue damage extending into the dermis. Fourth-degree frostbite involves severe tissue necrosis reaching muscle and bone, often leading to amputation. This severe stage is characterized by dark purple or black skin post-thawing.
Jazzt also discusses the physiological response to extreme cold, where arterioles constrict to preserve core body temperature, causing the skin to appear white due to reduced blood flow. Preventive measures include covering exposed skin to minimize heat loss and avoid frostbite. Early rewarming of affected tissue is critical for assessing damage and restoring blood flow, provided the damage is not extensive. This project visually demonstrates the different frostbite stages and emphasizes the importance of timely intervention and protection against cold exposure.