
My steam project will be covering the following objective, Knowing the structure of the knee joint. The knee is one of the largest and well-built joints in the body. There are three articulations of the knee joint which are, femoropatellar joint, medial tibiofemoral joint and lateral tibiofemoral joint. To form the knee joint, the lateral and medial condyles articulate with the tibia. The two articular discs are the medial meniscus and lateral meniscus which can be found between the articulating surfaces of the tibia and femur. The medial meniscus and lateral meniscus form the connection between the shin bone and thigh bone and are also made of fibrous cartilage. Both menisci are free to move during knee motions, however the medial meniscus appears to have less movement. “The menisci provide padding between the bones and help to fill the gap between the round femoral condyles and flattened tibial condyles. Some areas of each meniscus lack an arterial blood supply and thus these areas heal poorly if damaged” (Anatomy and physiology, pg. 385). The knee joint is held in place by multiple ligaments in the extended position. The collateral ligaments help maintain the knee against any bending and twisting stresses in the frontal plane. The anterior cruciate ligament and posterior cruciate ligament help maintain the knee against many movements of the tibia at the intercondylar eminence. The anterior cruciate ligament becomes compressed when the knee is extended resulting in resisting hyperextension whereas posterior cruciate ligament stops the femur from sliding anteriorly off the top of the tibia.
Considering that the knee joint is primarily supported by ligaments and muscles, any injury that were to occur will lead to knee instability. Uncontrolled rotating movement occurs when the knee is bent, the applied pressure all at the same time will lead to a shearing movement. “The meniscus is critical for load transmission, stabilization, shock absorption, and lubrication of the knee. It is estimated that the medial and lateral meniscus bear 50% and 70% of the load of the medial and lateral compartment individually” (Zhang, para 1). According to “the biomechanical changes of load distribution with longitudinal tears of meniscal horns on knee joint”, it is estimated that approximately 650,000 meniscus surgeries occur annually in the USA because of meniscal tears. There are three Layers of the meniscus which are the outer layer, the middle or lamellar layer, and the deep layer. The outer layer contains randomly aligned type 1 fibers. The middle or lamellar layer contains fibers that are more parallel in orientation and radial fibers located at the peripheral ends. Lastly, the deep layer has circumferentially oriented type 1 fibers and little amounts of radially oriented tie fibers.
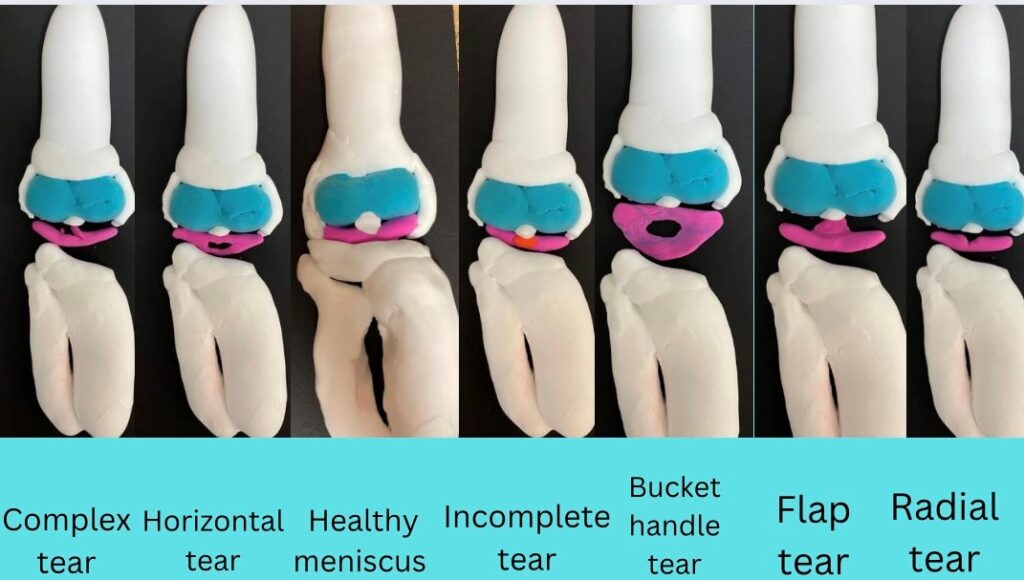
There are 6 different types of meniscal tears which are longitudinal also known as circumferential or vertical, radial, horizontal, incomplete, complex, and flap. “Longitudinal tear with centrally displaced inner fragment is referred as a “bucket handle” tear that is highly associated with pain, perceived instability, and mechanical locking” (Tarafder, para9). longitudinal tears involve the bigger portion of the meniscus, it occurs in the longitudinal direction down by the meniscus periphery. A radial tear occurs in the posterior portion of the medial meniscus. The radial tear is in the location of the knee where blood isn’t supplied therefore, it cannot heal on its own. A horizontal tear is also known as a cleavage tear, that runs parallel and horizontally to the tibial plateau. The flap tear is an oblique horizontal as well as vertical cleavage. Tears that occur in many planes are known as complex tears. According to the article of explant models for meniscus, “As per a previous study followed up total 198 patients, longitudinal tear is the most prevalent, accounting for ~46% of all tears, whereas radial, flap, and complex tears account for ~7%, ~4.5% and ~13%” ( Tarafder, para 9). There was another study along a radiographic follow up with a total of 155 patients that described how traumatic longitudinal tears “accounted for 42% and degenerative tears are 45% of all meniscus injuries” ( Tarafder, para 10). “Of the degenerative tears, total 32% were flap tears and horizontal and other tears were 13%” (Tarafder, para 10). Based on the evidence that was shown, each type of tear varies out of the tested patients’ populations.
Symptoms for a torn meniscus are swelling and severe pain that can occur up to 24 hours after the injury. Walking will be difficult, there will be pain when flexing or extending the knee. To diagnose a meniscal tear, doctors will ask general questions such as when the pain occurred and how the knee has been feeling since the injury. From there tests will commence, the tests will be physical exams with the doctor asking the patient to flex and extend, pivot, etc. After the physical examination, they will run an MRI to determine the diagnosis. The meniscus will appear black on the MRI and the white lines will indicate any tears. With radial tears, surgery may be required only if the tear is severe, the surgeon performing the surgery will cut away the damaged area of the meniscus. With a horizontal tear, rather than removing the part of the damaged meniscus the surgeon will attempt to sew the circumferential fiber together. An incomplete tear tends to be stable injuries and no surgery is required. A flap tear generates an unusual tear pattern and can be removed to resolve pain. A bucket handle tear requires immediate surgery to reestablish the bending ability of the knee. Bucket handle tears occur when the knee becomes locked and the part of the meniscus that is torn blocks the normal movement of the knee. Depending on the severity of the tears, Physical therapy may be the only requirement to support the healing process. If the MRI shows either grades 1 or 2 tears and the physical exam and symptoms do not appear consistent surgery will not be needed, they will refer you to physical therapy. If grade 3 meniscal tear were to occur, surgery will be required which may include: Arthroscopic total meniscectomy, Arthroscopic partial meniscectomy, or Arthroscopic repair.
Citations
Tarafder, S., Park, G., & Lee, C. H. (2020). Explant models for meniscus metabolism, injury, repair, and healing. Connective tissue research. Retrieved November 21, 2022, from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7190414/
Zhang, K., Li, L., Yang, L., Shi, J., Zhu, L., Liang, H., Wang, X., Yang, X., & Jiang, Q. (2019, July 25). The biomechanical changes of load distribution with longitudinal tears of Meniscal Horns on knee joint: A finite element analysis. Journal of orthopaedic surgery and research. Retrieved November 21, 2022, from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6659249/
Meniscus injuries: Types, causes, therapy. medi. (n.d.). Retrieved November 21, 2022, from https://www.medi.de/en/diagnosis-treatment/knee-pain/meniscus-injury/
Free textbooks online with no catch. OpenStax. (n.d.). Retrieved November 22, 2022, from https://openstax.org/details/books/anatomy-and-physiology
Mary’s project is about different types of meniscus tears. It describes the structure of the connective tissue that makes up the knee joint, and how ligaments and muscles support the knee in addition to the meniscus. Mary also describes the structure of the meniscus- it is made up of 3 different layers, and tears can occur in one or multiple layers. The media portion of this project demonstrates what different meniscus tears would look like, and what a healthy meniscus looks like. The essay describes how injury to the meniscus can occur- usually by rotation of the knee paired with pressure, which causes a shearing motion that can tear the fibrous cartilage of the meniscus. Mary’s essay also describes symptoms of a tear, including pain and swelling, and how a meniscal tear can be diagnosed via radiologic imaging.