
For this STEAM project, I chose to research Diastasis Recti Abdominis and possible therapeutic solutions. The course objective I have explored through this project is to “Explain common disorders during pregnancy and their cause.”
My inspiration for this project came from my mom’s experience with pregnancy and delivery of my two sisters and me. Diastasis Recti Abdominis “or rectis diastasis is an acquired condition in which the rectus muscles are separated by an abnormal distance along their length, but with no fascia defect.” Some defining characteristics of Diastasis recti abdominis include “a protruding midline as a result of an increase in intra-abdominal pressure.” Anatomically what this accumulates in is “a gradual thinning and widening of the linea alba, combined with a general laxity of the ventral abdominal wall muscle.” (Cavalli 2021). This potential leads to complications and “risk factors for the actual development of midline hernias (umbilical, epigastric, trocar and incisional hernias) due to deterioration of the connective tissue and pulling of the abdominal muscles.” (Cavalli 2021). Even still, “diastasis recti is extremely common in those who are pregnant and during the postpartum period” which is about “60% [of pregnant women]”. (Cleveland Clinic 2022) What’s interesting though is that ‘within eight weeks of delivery and usually resolves itself yet “40% of those who have diastasis recti still have it by six months postpartum.” (Cleveland Clinic 2022).
As shown previously, Diastasis Recti Abdominus is a common disorder during pregnancy and even after pregnancy, it continues to be a prevalent disorder after birth. More specifically, “Long-lasting increased intra-abdominal pressure from a growing fetus and expanding uterus combined with hormonal changes (increasing in secretion of relaxin, progesterone, and estrogen) on connective tissue create a physiological (normal) widening of the IRD, creating a DRA during pregnancy”(Cavalli 2021). Risk factors for DRE include: “pregnancy (the resulting hormonal changes, the increased size of the uterus, anterior pelvic tilt with or without lumbar hyperlordosis, the increased intraabdominal pressure), cesarean section, multiple pregnancies, fetal macrosomia, as well as genetically-conditioned defects in collagen structure (including congenital disproportion of the collagen III/I ration), considerable body mass losses occurring spontaneously or after bariatric surgeries, abdominal surgical procedures. Nevertheless, certain studies “reported no association between DRA and the pre-pregnancy body mass index, weight gain, a baby’s birth weight or abdominal circumference, heavy lifting, lifting and carrying children, and regular exercise” (Michalska et al 2018).
If Diastasis recti persists, physiotherapy and, in rare cases, surgery are the main treatment methods. This is “considered to be the only treatment method that may decrease IRD” (Michalska et al 2018), inter-recti distance. Many “studies confirm the positive influence of exercises on reducing the inter-recti distance” but generally no “acceptable protocol of therapeutic exercises has been formulated so far” (Michalska et al 2018). Although we know that physiotherapy has positive effects on decreasing IRD, it is not known “which abdominal exercises are the most effective” but “the most commonly applied are: an abdominal exercise programme (strengthing of transversus abdominis muscle or rectus abdominus muscle), a postural training, education and training on appropriate mobility techniques and lifting techniques, methods of strengthening transverse abdominis muscles (Pilates, functional training, the Tupler’s technique exercise with or without abdominal splinting), the Noble technique (manual approximation of rectus abdominis muscles during a partial sit-up), a manual therapy (soft tissue mobilization, myofascial release), abdominal bracing and taping, the tubigrip or a corset” (Michalska et al 2018). With that being said, women with DRA must be cautious and pursue professional medical assistance in treatment because certain abdominal exercises can exacerbate DRA. Specifically, “any movement that bulges the abdominal wall forward can cause more damage to your diastasis recti”, which includes “everyday movements like getting out of bed or up off a chair” (Cleveland Clinic 2022). This requires women to be mindful, seek professional help and avoid exercise like, “crunches or sit-ups of any kind, planks or push-ups” or “any exercise that causes your abdominals to bulge, cone or dome” (Cleveland Clinic 2022). With that being said, “the best exercises for diastasis recti are those that engage the deep abdominal” which “involve deep breathing and slow, controlled movements” (Cleveland Clinic 2022).
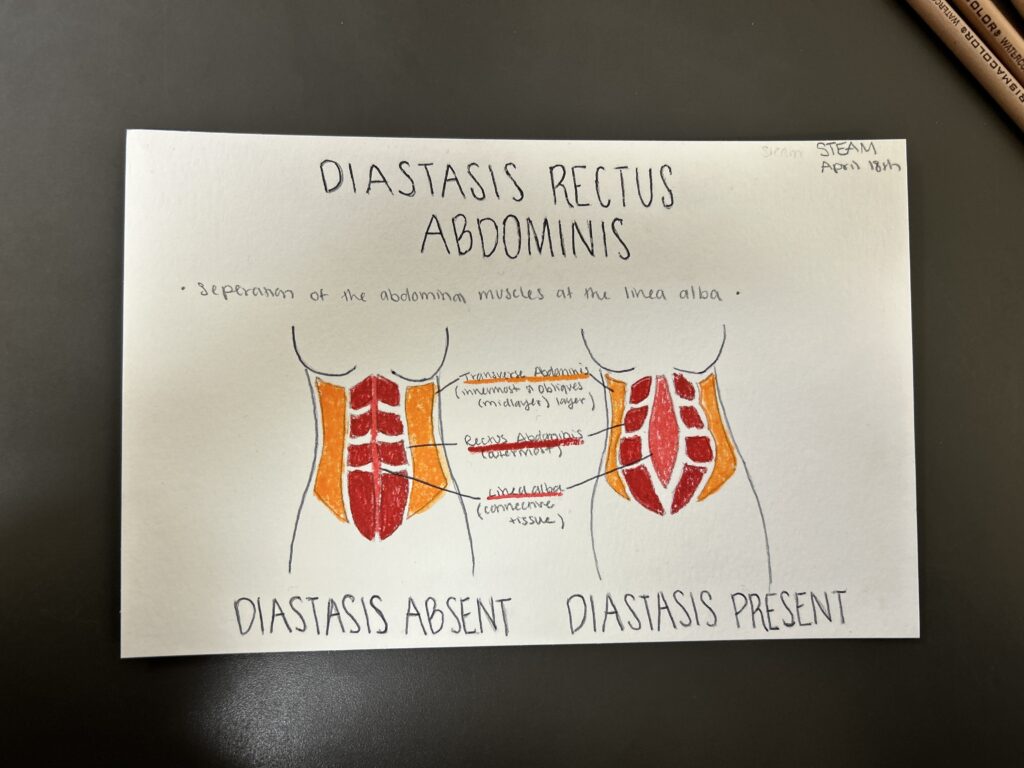
The purpose of my watercolor painting diagram is to note the physical change in anatomy that is undergone when a woman becomes pregnant and develops diastasis rectus abdominis. Present in this diagram are the transverse abdominis, rectus abdominis, the linea alba, and the internal and external obliques. The most noteworthy detail of the diagram is the separation of the rectus abdominis at the linea alba resulting in Diastasis rectus abdominis.
Picture of Process:
Watercolor Diagram Product:
Sources:
Michalska, A., Rokita, W., Wolder, D., Pogorzelska, J., & Kaczmarczyk, K. (2018). Diastasis recti abdominis—a review of treatment methods. Ginekologia polska, 89(2), 97-101.
Cleveland Clinic medical professional. “Diastasis Recti (Abdominal Separation): Symptoms & Treatment.” Cleveland Clinic, Cleveland Clinic, 8 Feb. 2022, my.clevelandclinic.org/health/diseases/22346-diastasis-recti.
Cavalli, M., Aiolfi, A., Bruni, P. G., Manfredini, L., Lombardo, F., Bonfanti, M. T., … & Campanelli, G. (2021). Prevalence and risk factors for diastasis recti abdominis: a review and proposal of a new anatomical variation. Hernia, 25(4), 883-890.
This project covers Diastasis Rectus Abdominus which is a condition identified by the abnormal separation of the abdominus rectus muscles with no fascia defect. This is a common condition which often affects pregnant and post-partum women. Diastasis Rectus Abdominus in pregnant women is thought to be caused as a result of hormonal changes such as increased relaxin and increased intra-abdominal pressure from a growing fetus and expanding uterus. These changes are thought to loosen the connective tissue like the linea alba around the abdominus rectus muscles allowing the muscles to be pulled away from the midline of the body.
Treatments for Diastasis Rectus Abdominus include physical therapy and surgery if necessary. Often times the condition resolves itself within six months of giving birth, but it is not uncommon for the condition to not resolve on its own. In the latter case physical therapy which usually consists of controlled core exercises under professional supervision can improve symptoms. If the condition still persists after physical therapy or is severe, surgery can be done in order to repair the muscles and surrounding connective tissues.