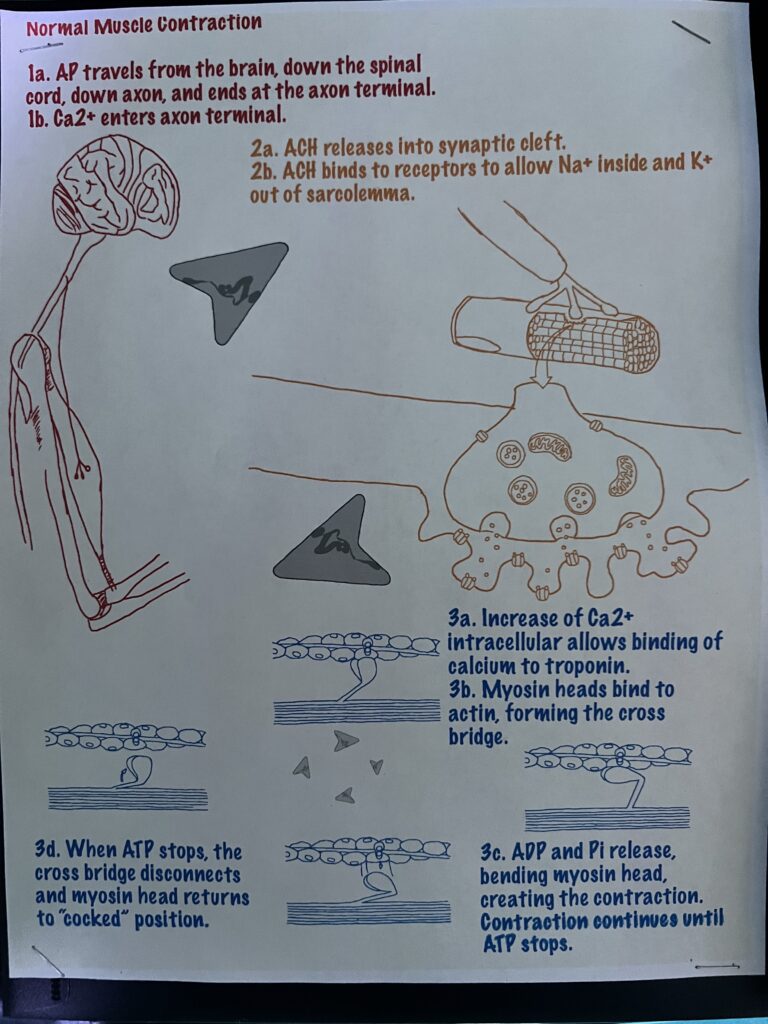
My objective is to describe how a muscle contraction is induced. A typical muscle contraction begins with an action potential (AP) sent from the brain and travels down the spinal cord, through a motor neuron, and down an axon. As it continues down, it meets the axon terminal. This signal or AP allows calcium channels to open, allowing calcium to enter the neuron. With a normal contraction, acetylcholine (ACH) is released inside the synaptic cleft. These neurotransmitters attach to ion receptors opening them. Na+ flows into the sarcolemma as K+ flow outwards. There is a ratio of 3:2 ratio of Na+ to K+, producing a local charge in the membrane potential called end plate potential. Then ACH diffuses away, and the ion channel closes. Sarcoplasmic reticulum release Ca2+ to cytosol. This allows for Ca2+ to bind to troponin, enabling it to change shapes. This moves the troponin away, allowing the myosin head to bind to the actin filament. ATP powers this cross bridge, so when ADP and Pi are released, they pull the myosin head down and forward. At this point, a contraction occurs. As long as there is ATP, there is a contraction. Once ATP stops, the myosin head detaches from the actin filament. Next, myosin breaks down ATP to ADP and Pi, and the myosin head returns to its normal “cocked” position.
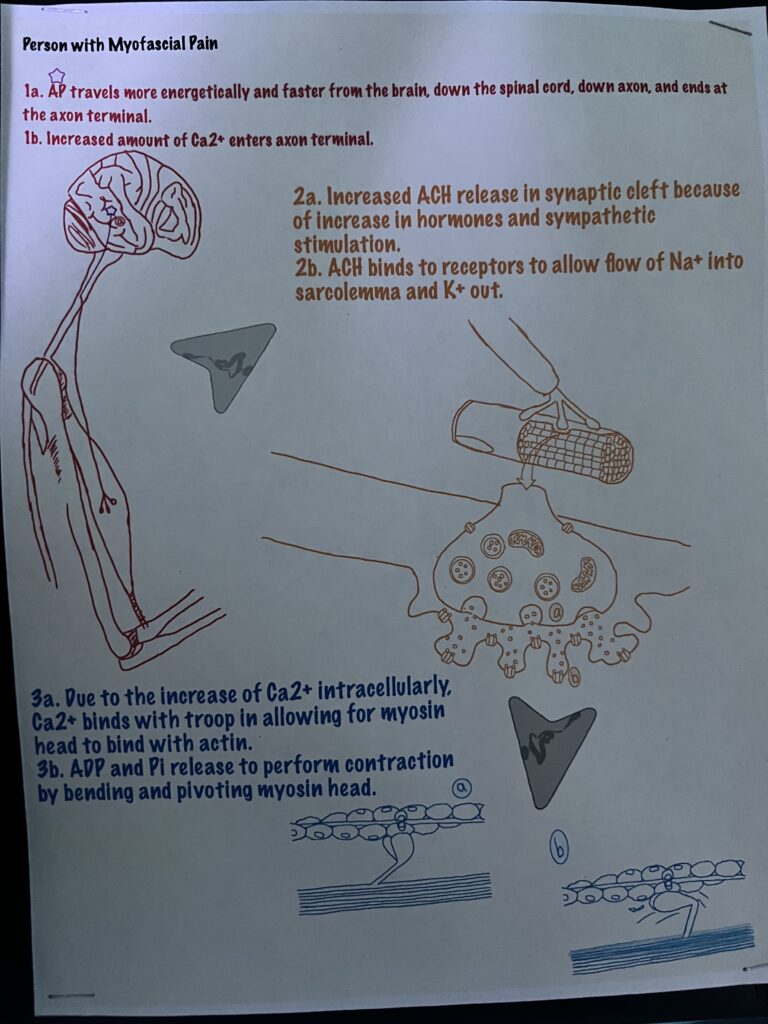
A condition called Myofascial Pain Syndrome, causes an increase in calcium to flood inside the neuron. Patients have painful contractions in areas called myofascial trigger points. These contractions or impulses are caused by spontaneous electrical activity that generates an action potential and can last for some time. This, then, can cause an increase in the amount of Ca2+ released from the sarcoplasmic reticulum, causing muscle hypercontracture. Muscle hypercontracture is essentially the excessive contraction of a muscle fiber. A study on the characterization of hypercontracture fibers in domestic turkeys showed, under a microscope, a high activity of Ca2+ – ATP reaction. The spontaneous AP that is generated carries a charge that releases an excess of Ca2+ inside the axon. With an intracellular increase of Ca2+, the effects can travel down to cause a contraction. More Ca2+ generates a concentric contraction. Myofascial trigger points are most common under psychological stress conditions and release an increase of ACH. This is caused by hormones and sympathetic stimulation released because of psychological stress. Researchers show that because of the rise in tension that the muscle fiber undergoes creates a taut band. This band constricts blood flow and reduces oxygen to the muscle fiber. As the muscle fibers go into distress, they send pain signals back up to the brain. This signals for autonomic modulation, which turns and causes the abnormal release of ACH. Treatments for pain are treated with either pharmacological or non-pharmacological methods. This includes anti-inflammatory medications or regular massages. A technique that has become the standard of practice is soft tissue needling. Here they inject a patient with either anesthetics and/or steroids through a 30-gauge needle.
References
Gerber, N. L., Sikdar, S., Hammond, J., & Shah, J. (2011). A brief overview and update of myofascial pain syndrome and myofascial trigger points. J. Spinal Res. Found. Spring, 6.
Jafri, M. S. (2014). Mechanisms of myofascial pain. International Scholarly Research Notices, 2014, 1–16. https://doi.org/10.1155/2014/523924
Sosnicki, A., Cassens, R. G., McIntyre, D. R., Vimini, R. J., & Greaser, M. L. (n.d.). Characterization of hypercontracted fibers in skeletal muscle of domestic turkey (Meleagris gallopavo). DigitalCommons@USU. Retrieved November 22, 2022, from https://digitalcommons.usu.edu/foodmicrostructure/vol7/iss2/4