
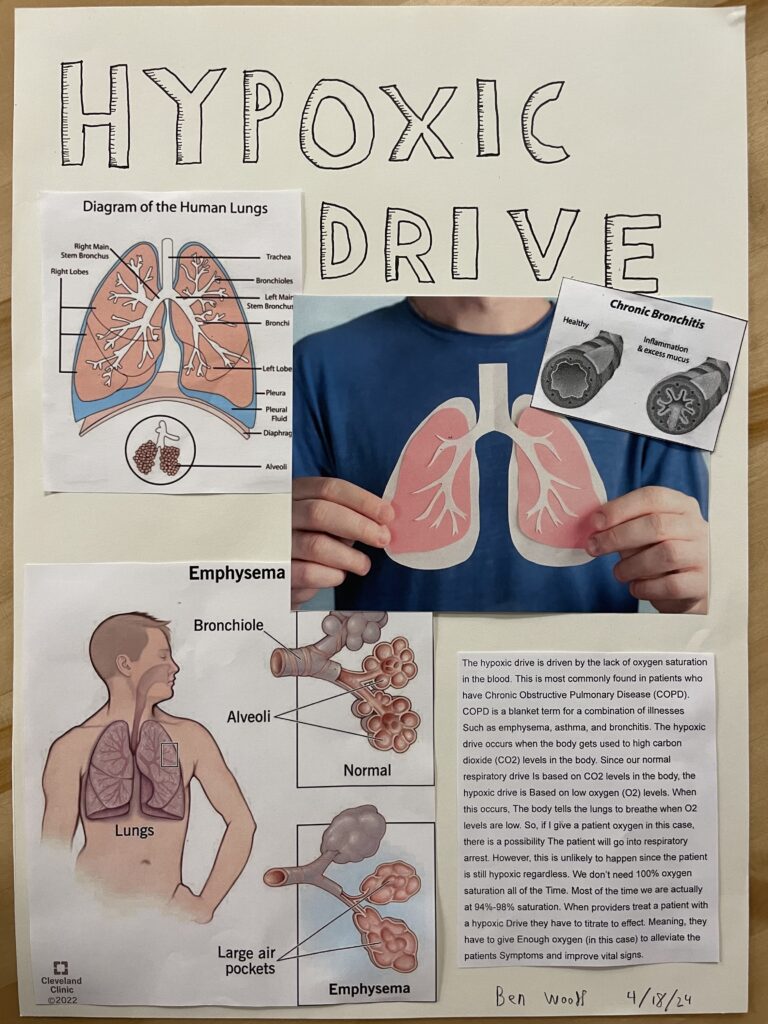
My STEAM project is on the hypoxic drive. In healthy people with no respiratory issues, our normal respiratory drive is based off of Carbon-Dioxide (CO2) levels in the body. If we have too much CO2 in the body then we’ll adjust our ventilations to off-load the excess CO2. In people who have Chronic Obstructive Pulmonary Disease (COPD) they have and maintained a state of high CO2 levels in the body. At some point their body has gotten used to having high CO2 levels and started to breathe based off of oxygen levels instead of CO2 which is called the hypoxic drive. The hypoxic drive is when the person breaths when they don’t have enough oxygen. As a provider, if I give oxygen to a patient with a hypoxic drive who is experiencing shortness of breath I run the risk of respiratory failure because I’ve meet their oxygen demand, thus the patient doesn’t inhale again. If a person has other illnesses that exacerbate COPD then that may very well happen. With all of this in mind, the patient is still overall hypoxic so they will need oxygen, just not all of it. I can titrate to effect which means I can give enough to make their condition better but I don’t need to make them 100% saturated with oxygen. In fact, most of us don’t stay 100% saturated with oxygen, we usually stay within the 94-98% range. As a provider who’s treating a patient with this condition, I need to target their oxygen saturation to around 92-96% and that’s just in the pre-hospital world. I need to get them stable for transport if possible and if not then I need to get to the hospital as fast as I can while trying to get them oxygenated. If all else fails I can still ventilate for them via Bag-Valve-Mask (BVM).
Here’s me working on my artwork and my essay for the STEAM project.
