
Objective 10: Describe how ovulation, menses, pregnancy, and spermatogenesis are hormonally regulated.
Gender affirming hormonal therapy (GAHT) is a hormonal therapy with the goal to align a person’s physical characteristics with their gender identity when that identity does not match the assigned birth sex. As of 2020, 1.4 million people identify as transgender or non-binary (Taub et al., 2020), or 0.5% of the general population (Ahmed and Leinung, 2017).
The primary GAHT for transgender males is the administration of testosterone by transdermal application or intramuscular injections. The goal is to transition to a physical body that is in alignment with the person’s gender identity. Testosterone is a steroid hormone naturally occuring in high amounts in cisgender males, and is important for the “development of the testicular reproductive system, the maturation of sperm cells, and the development of secondary sex characteristics such as a deepened voice, body hair, and increased muscle mass.” (Betts et al., 2022). The goal of the administration of testosterone to transitioning males is to develop the secondary sex characteristics as well as the cessation of the menstrual cycle. The menstrual cycle is a defining pillar of the secondary sex characteristics of cisgender females, and the repeated menstrual cycle for a transgender male is “a source of significant psychological stress.” (Ahmad). Additionally, the cessation of menstruation in transgender males has social implications in the need for education about unintended pregnancy and effective contraception (Taub et al., 2020).
Two important benchmarks serve as goals in GAHT – target testosterone levels that are comparable to cisgender males, and the cessation of menstruation. A study by Muir, Jones, and Man (2024) found that transmasculine patients were able to achieve target testosterone levels of >10 nmol/L within a median time of 4 months, which is the standard cisgender male testosterone level. In addition to testosterone levels, the study also noted that sustained administration of testosterone was shown to increase hemoglobin and hematocrit levels (Muir et al. 2024).
Testosterone as a GAHT is an effective treatment for the cessation of the menstrual cycle, and high doses are not typically necessary to suppress the menstrual functions (Ahmad). The research by Ahmed and Leinung (2017) found that a low dose (20-40 mg weekly) of intramuscular testosterone resulted in 55% of patients having cessation of menses within 6 months, while 32% had cessation in 6-12 months. Though the ovaries do produce a small amount of testosterone (0.7mg per 24 hours) it is 10 times less than cisgender males (Pirtea et al., 2021).
GAHT testosterone was shown to have noticeable effects on the functions of the ovaries after 6 months of treatment, as well as atrophic effects on breast tissue in long term usage (Pritea et al., 2021). Pritea et al. (2021) found that after 21 months of GAHT testosterone, the ovaries of patients were enlarged with a thickened collagenous cortex, increased antral follicles, increased cystic atretic follicles (a follicle that fails to develop and dies), and luteinization of the connective tissue supporting the follicles (stroma).
Sex hormone changes also occur as a result of GAHT with testosterone. Subjects that were prescribed testosterone for at least one year showed different hormone levels of estradiol, luteinizing hormone (LH), and follicle stimulating hormone (FSH) compared to both cisgender males and cisgender females (Greene et al., 2020). Testosterone levels were comparable to cisgender males, and prolactin levels were comparable to cisgender females (Greene et al., 2020).
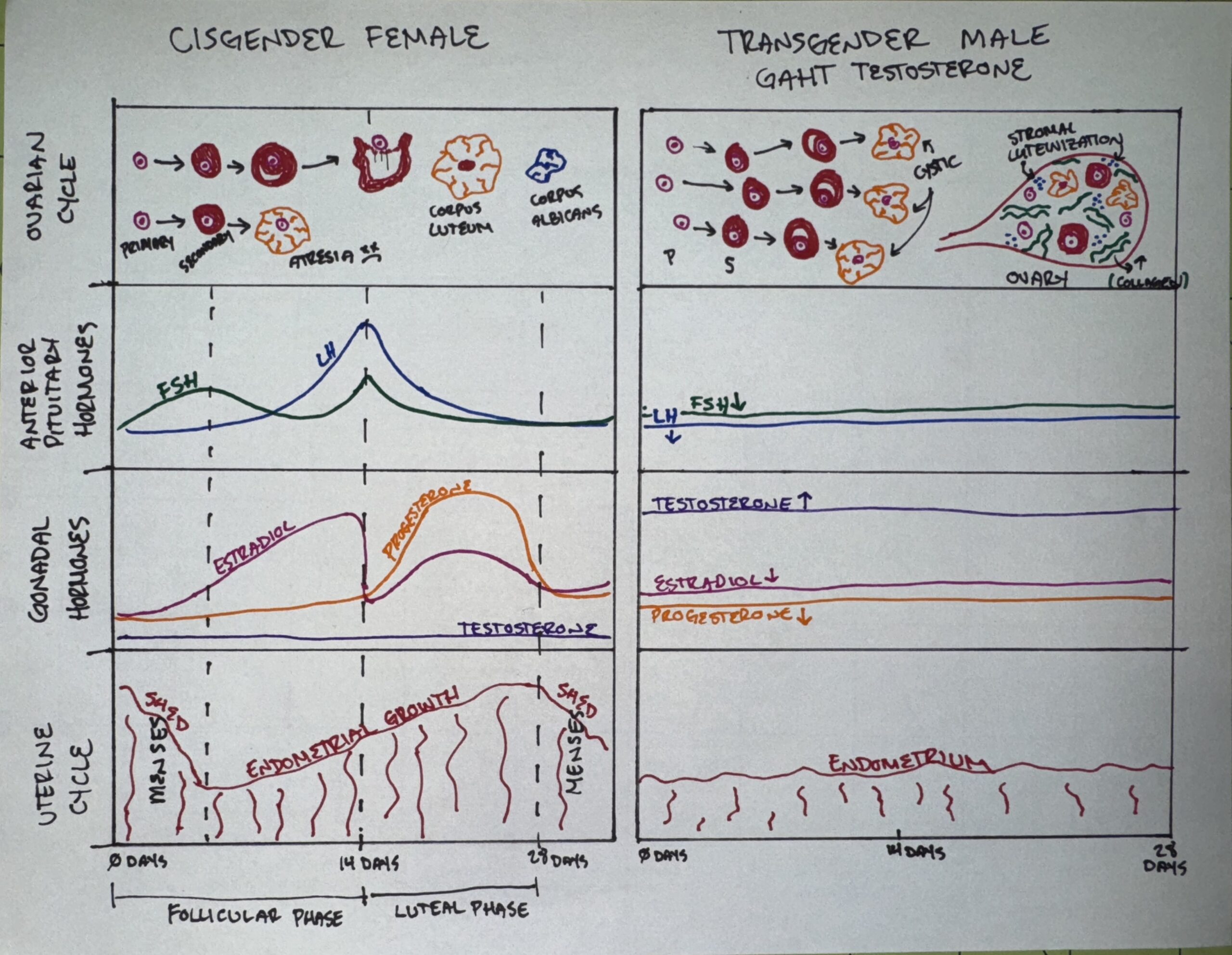
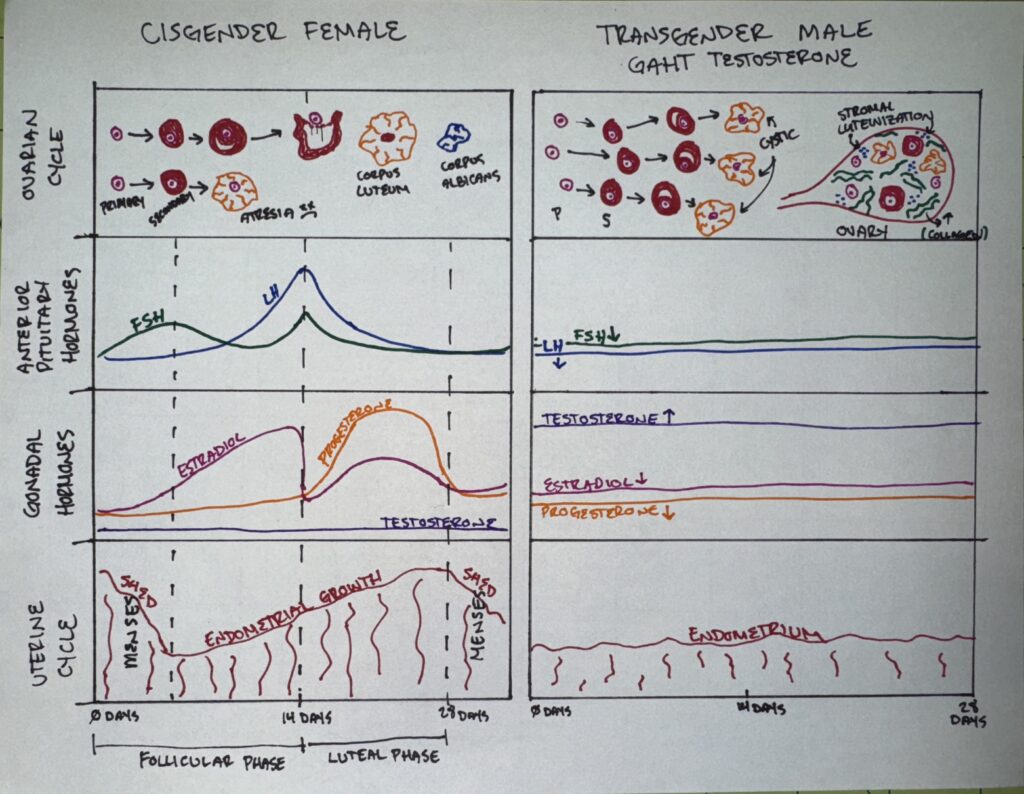
As increases in testosterone levels have physiological effects (masculinization), the resulting decreases in estrogen, LH, and FSH lead to the cessation of the menstrual cycle. High levels of testosterone rapidly induce hypothalamic-pituitary-gonadal suppression which leads to anovulation and ovulatory dysfunction (Taub et al., 2020). FSH and LH are secreted by the anterior pituitary, during the follicular phase of the cycle suppression of the release of FSH would restrict the growth of follicles in the ovaries and increase follicular atresia, and the suppression of LH would prevent granulosa and theca cells from producing estrogen. The lack of estrogen would prevent the endometrium of the uterus to thicken. In the ovulation stage of the cycle, the lower levels of LH would not be enough to trigger ovulation. Without ovulation, there is no corpus luteum to produce progesterone and those hormonal levels remain low during the luteal phase.
GAHT is an effective treatment for the masculinization of transgender men, and is shown to successfully suppress the menstrual cycle without the need for invasive surgery.
References
Ahmad, S., & Leinung, M. (2017). The Response of the Menstrual Cycle to Initiation of Hormonal Therapy in Transgender Men. Transgender Health, 2(1), 176–179. https://doi.org/10.1089/trgh.2017.0023
Betts, J. G., Young, K. A., Wise, J. A., Johnson, E., Poe, B., Kruse, D. H., Korol, O., Johnson, J. E., Womble, M., & DeSaix, P. (2022, April 20). Anatomy and Physiology 2e | OpenStax. Openstax.org; OpenStax. https://openstax.org/books/anatomy-and-physiology-2e/pages/1-introduction
Greene, D. N., Schmidt, R. L., Winston-McPherson, G., Rongitsch, J., Imborek, K. L., Dickerson, J. A., Drees, J. C., Humble, R. M., Nisly, N., Dole, N. J., Dane, S. K., Frerichs, J., & Krasowski, M. D. (2020). Reproductive Endocrinology Reference Intervals for Transgender Men on Stable Hormone Therapy. The Journal of Applied Laboratory Medicine. https://doi.org/10.1093/jalm/jfaa169
Pirtea, P., Ayoubi, J. M., Desmedt, S., & T’Sjoen, G. (2021). Ovarian, breast, and metabolic changes induced by androgen treatment in transgender men. Fertility and Sterility, 116(4), 936–942. https://doi.org/10.1016/j.fertnstert.2021.07.1206Taub, R. L., Ellis, S. A., Neal-Perry, G., Magaret, A. S., Prager, S. W., & Micks, E. A. (2020). The effect of testosterone on ovulatory function in transmasculine individuals. American Journal of Obstetrics and Gynecology, 223(2), 229.e1–229.e8. https://doi.org/10.1016/j.ajog.2020.01.059
This steam project uses the medium of hand drawn charts showing the difference testosterone makes when injected into a female transitioning to a male body. This chart includes graphs on the levels in a CIS female body versus a transgender male body once testosterone has been injected. The graphs include information on the uterine cycle, gonadal hormones, anterior pituitary hormones, and the ovarian cycle.
The essay portion of the STEAM project gives an in-depth overview of the two main objectives of hormone therapy: physical body alignment with the sex the person identifies as and cessation of the menstruation cycle. Something I found really fascinating in the essay was that patients were found to have been able to achieve testosterone levels “of >10 nmol/L within a median time of 4 months, which is the standard cisgender male testosterone level.” The essay also gives the results that the menses cessation can happen as quickly as the first six months. After reading this essay and seeing the graph on the chart side by side it really puts into perspective what female to male transgender people go through without surgery. It’s incredible what hormone therapy can accomplish. I also really appreciated the mention of how important it is for the transitioners mental health to be accounted for. Changing your body but still having a menstrual cycle and not being able to fully and completely be the sex you identify as would be incredibly damaging to your psyche.