
Objective
Describe the onset, symptoms, and recovery of Parsonage-Turner Syndrome (PTS). To teach the reader how PTS restricts nerve conduction and can cause pain, myopathy, and atrophy.
Introduction
In 1948, Parsonage-Turner Syndrome was named after English physicians, Parsonage and Aldren Turner, who identified 136 soldiers with similar symptoms. These soldiers experienced severe shoulder pain, paralysis, scapular winging, and muscle weakness. The onset is rapid with severe pain, causing most victims to experience sleep disturbances. It is unclear exactly why PTS occurs but it is most common in patients who have experienced infection, coronavirus, surgery, and vaccination. It is understood to be an inflammatory autoimmune response that attacks the long thoracic nerve and brachial plexus.
Recovery is a slow process depending on the severity of the injury. “Upper trunk injuries did best for recovery with near-complete functional recovery by 1 year in most. In contrast, lower and middle-trunk (hand and forearm) involvement typically did not normalize until 1.5 to 3 years” (Meiling, 2024). The initial goal is pain management which is best accomplished with anti-inflammatory steroids such as prednisone. Within a couple of weeks, when the range of motion is regained, physical therapy must begin to improve the ability to accomplish everyday activities. Due to muscle weakness of the affected muscles, patients must be cautious of muscle strains, subacromial bursitis, rotator cuff tendinopathy, and subpectoral impingement that can occur due to other muscles overcompensating.
Nerve Conduction
The process of nerve conduction is as follows; 1) the neuron is at rest with the inside of the neuron being negatively charged, 2) stimulus occurs and depolarizes the neuron, 3) an action potential is initiated and shoots down the axon, 4) sodium channels close and potassium channels open and repolarization begins, 5) the membrane becomes more negative than the resting potential, and 6) the sodium-potassium pump restores the resting membrane potential.
When the nerves swell it can cause damage to the myelin sheath and nerve axons. The myelin sheath has myelinating glial cells that wrap several layers of cells around the cell membrane of an axon segment. This protects and insulates the axon segment, allowing electrical impulses to travel quickly along the nerve. When this myelin sheath is damaged it disrupts and slows the nerve impulses, causing pain, atrophy, and sensory loss. In a study about PTS, we find, “The authors reported acute motor axon loss signs, normal latencies with an important reduction of compound action potentials (CMAP) amplitude, signs of subacute plexopathy, and… In addition, a few patients also presented an absence of sensory responses or reduced sensory nerve activation potential amplitude” (Alvarado, Lin-Miao, Carrillo-Arolas, 2023).
Conclusion
Nerve pain sucks. The autoimmune inflammatory reaction causes damage to the nerve tissue causing severe pain and muscle weakness. It limits day-to-day activities and changes the way one lives their life. Once the pain is manageable, physical therapy and healthy living can hopefully heal most of the damage and return one’s strength. Parsonage-Turner’s Syndrome is still being studied and hopefully, medical professionals will be able to understand the cause and cure for it fully.
Art Project
Photo #1 is a drawing of the brachial plexus which is a network of nerves that connect the spinal cord to the arm. It connects C5, C6, C7, C8, and T1 to the nerves of the arm which carries movement and sensory signals. Parsonage-Turner Syndrome affects any of these nerves, commonly affecting the deltoid, rotator, cuff, serratus anterior, biceps brachii, and triceps brachii.
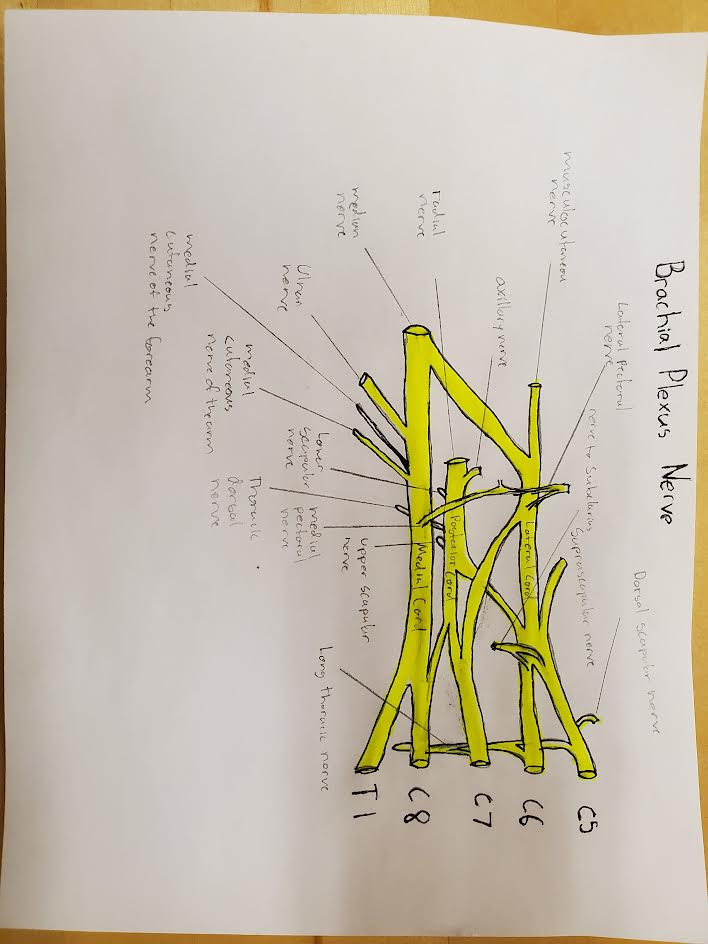
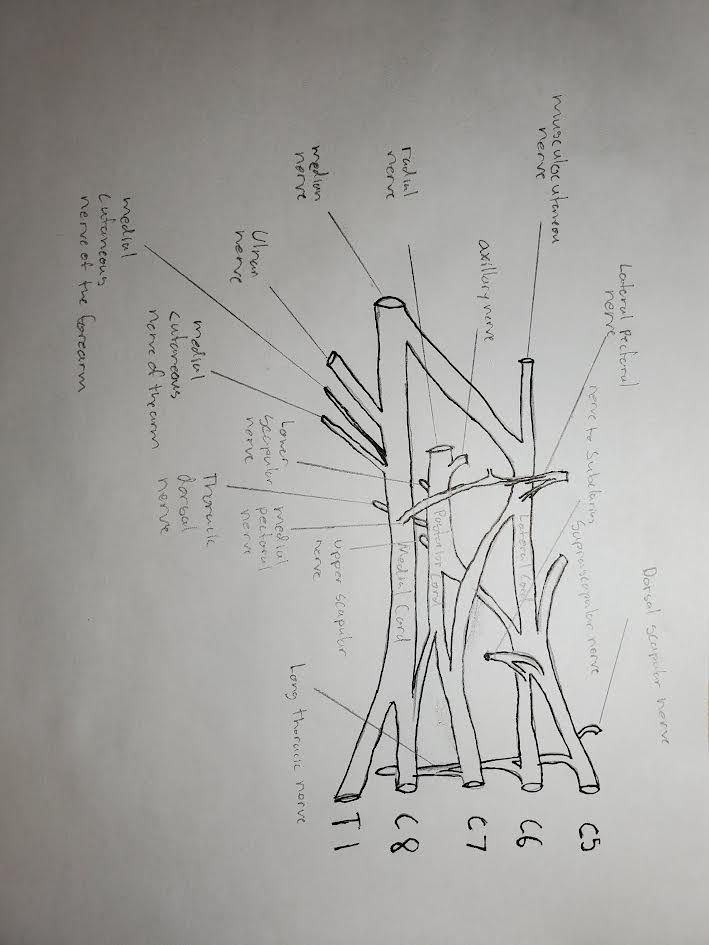
Photo #2 is my drawing, partially complete.
Here is a photo of me completing my drawing of the brachial plexus.
The End…
Works Cited
Ameer, Muhammad Zain, et al. “Association of Parsonage-Turner Syndrome with Covid-19 Infection and Vaccination: A Systematic Review.” The Journal of International Medical Research, U.S. National Library of Medicine, July 2023, pmc.ncbi.nlm.nih.gov/articles/PMC10392513/#abstract1.
Cornea, Amalia, et al. “Parsonage-Turner Syndrome Following SARS-COV-2 Infection: A Systematic Review.” Biomedicines, U.S. National Library of Medicine, 9 Mar. 2023, pmc.ncbi.nlm.nih.gov/articles/PMC10045449/#B26-biomedicines-11-00837.
“Mayo Clinic Proceedings.” Mayo Clinic Proceedings | Journal | ScienceDirect.Com by Elsevier, www.sciencedirect.com/journal/mayo-clinic-proceedings. Accessed 18 Nov. 2024.
Parsonage-Turner Syndrome and Hereditary Brachial Plexus Neuropathy
Meiling, James B. et al.
Mayo Clinic Proceedings, Volume 99, Issue 1, 124 – 140
Hey Samuel! I enjoyed reading your steam project, here’s my description of your project. In your project, you’re describing Parsonage-Turner Syndrome (PTS). PTS is a rare neurological disorder that primarily affects the brachial plexus, a network of nerves that extends from the spinal cord to the shoulder, arm, and hand. This condition is characterized by a sudden onset of severe shoulder pain, which is often debilitating and can significantly disrupt sleep and daily activities. Following the initial pain phase, individuals typically experience muscle weakness, paralysis, and atrophy, particularly affecting muscles such as the deltoid, rotator cuff, serratus anterior, biceps brachii, and triceps brachii.
The precise cause of PTS remains unknown, but it is believed to be an autoimmune inflammatory response. It has been observed more frequently in individuals who have recently experienced infections, undergone surgeries, or received vaccinations. The inflammation associated with PTS targets the long thoracic nerve and components of the brachial plexus, leading to nerve damage.
Recovery from PTS is generally slow and varies depending on the severity and specific location of the nerve injury. Upper trunk injuries tend to have a better prognosis, with many patients achieving near-complete functional recovery within a year. In contrast, injuries involving the lower and middle trunks may take between 1.5 to 3 years for significant improvement.
Management of PTS initially focuses on controlling pain through anti-inflammatory medications such as prednisone. As the acute pain subsides and range of motion improves, physical therapy becomes essential to restore function and prevent secondary complications like muscle strains and tendon issues due to compensatory movements.
Nerve conduction is impaired in PTS due to swelling and damage to the myelin sheath, which insulates nerve axons. This disruption slows electrical impulses, resulting in pain, sensory loss, and muscle atrophy. Studies have shown signs of acute motor axon loss and reduced compound action potentials, indicating subacute plexopathy. Ongoing research aims to deepen the understanding of PTS’s pathophysiology and improve therapeutic approaches, offering hope for more effective management and recovery strategies in the future.