

Huntington’s Disease: A Triplet Repeat Disorder
Introduction:
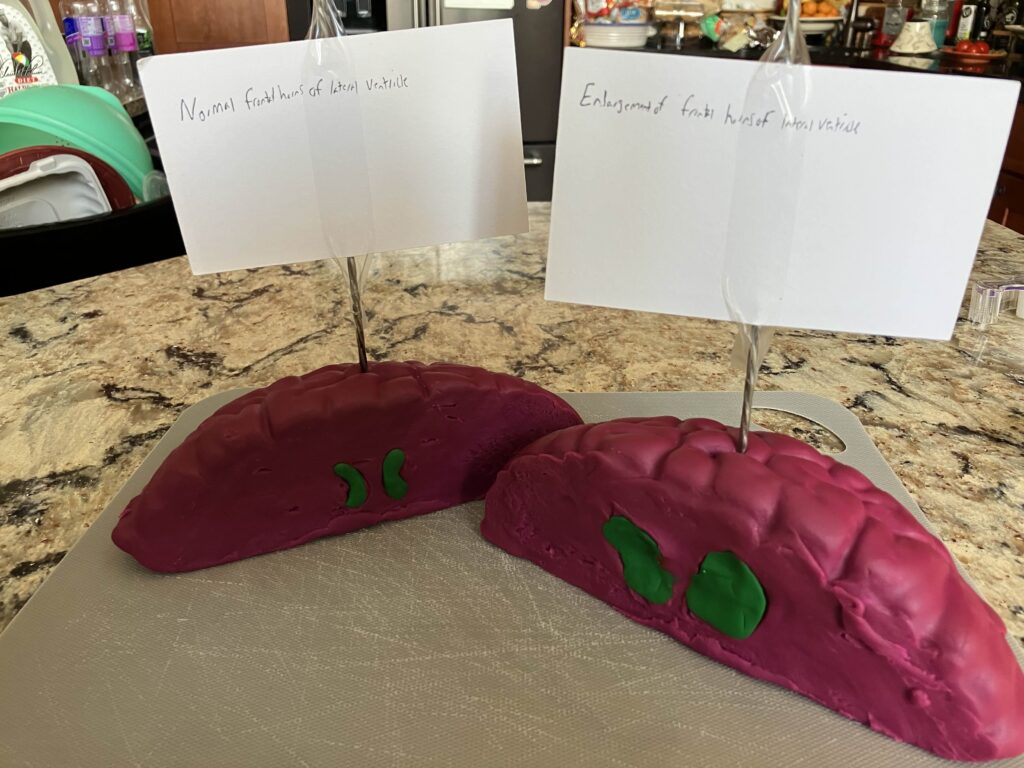
For my STEAM project, I have chosen to explore the components and structures of the nervous system through the lens of Huntington’s Disease (HD). Although the disease has been recognized since the early 1600s, it was formally identified in 1872 by George Huntington (Lanksa et al., 2000). HD is a progressive neurodegenerative triplet repeat disorder that exhibits genetic anticipation, meaning the disease worsens over time and in successive generations, and involves repeated sequences of three DNA bases (Consortium et al., 2019). This condition leads to the degradation of neurons in the brain, expansion of the frontal horns of the lateral ventricles, and impairment of motor and cognitive functions (Sharma et al., 2024).
The underlying cause of HD is a mutation in the huntingtin gene (HTT), which is crucial for physiological functions such as axonal trafficking (process by which proteins and other molecules are transported along nerve cells) and gene transcription regulation (process of controlling which genes are turned on and off in a cell) (Schulte et al., 2011). This mutation results in multiple polyglutamine repeats (glutamine being the amino acid encoded by CAG) and the aggregation (clumping) of misfolded proteins. Excessive aggregation disrupts neural pathways essential for movement and cognition, leading to neuron death.
HD is an autosomal dominant disorder, meaning it is inherited from one parent and requires only one copy of the mutated gene to manifest. With an average onset age between the late 30s and mid-40s and a survival time of 15 to 18 years post-onset (Caron et al., 1998), the disease allows individuals to pass it to their offspring. Symptoms typically include chorea (uncontrolled erratic movement of the body), cognitive decline, and behavioral changes. As HD progresses, individuals experience greater impairments, leading to a reduced quality of life and life expectancy. Current treatment strategies focus on slowing disease progression, alleviating symptoms, and improving care for those affected.
HTT location and polyglutamine length determination in severity and onset:
HTT is located at 4p16.3 (chromosome 4, p arm, loci 16.3) (Andhale, 2022). Located within the first exon exists several CAG (Glutamine) repeats. With CAG repeats of 6-35 being indicative of a regular unaffected person, 36-75 is indicative of an adult onset, and 48-121 repeats are indicative of juvenile onset (Brinkman et al., 1997). Triplet repeat disorders are due to slippage during DNA replication where DNA polymerase dissociation occurs (Viguera et al., 2001). The newly synthesized strand realigns with the template strand at the incorrect location, and the DNA polymerase will then add more nucleotides than originally intended. The protein created from this gene may fold incorrectly due to the repeats affecting the length and folding patterns.
Neuronal targets of HD:
The primary target of HD is striatal neurons, which are neurons located in the striatum and are associated with motor function. As mentioned prior, HTT produces huntingtin protein, which is a heavily utilized protein involved in striatal projection (neural pathways extending from the striatum) (Burrus et al., 2020). The mutated huntingtin protein form inclusion bodies (aggregates of protein) by aggregating around the exon 1 N-terminus around where the expanded CAG repeats are located (Chen et al., 2017). These inclusion body aggregates, with their expanded polyglutamine, induce apoptosis (planned neuronal death) in neuronal cells, in mostly striatal neurons (Sawa et al., 2003). It is postulated that striatal cells are more susceptible to death by HD due to a variety of reasons including mitochondrial dysfunction as striatal neurons possess high energy requirements for metabolic function, medium spiny neurons within the striatum are more susceptible to the cytotoxic effects of HD due to their unique physiology, and that striatal neurons accumulate more toxic aggregates of misfolded huntingtin protein as a faster rate. As neurons do not undergo mitosis, excessive loss of neurons has a profound impact on individuals.
Diagnosis and treatment of HD:
HD can affect youths as young as 12, although the medium onset is between late 30s to mid 40s. HD is generally diagnosed in individuals who exhibit motor and cognitive decline starting in their late 30s (jitkumar et al., 2024). Individuals may exhibit chorea, behavioral changes such as irritability and poor attention, and cognitive decline especially regarding the ability to multitask and plan. Secondary symptoms that can accompany HD include seizures in youths, slowed eye movement specifically in regards to tracking the movement of items, and ataxia (lack of muscle coordination). A blood test followup can look for increased polyglutamine repeats and lead to an accurate diagnosis.
Currently there is no cure for HD. The most common causes for death among patients manifesting HD are pneumonia, other infections, and suicide (Van Duijin et al., 2021). Instead current treatments focus on alleviation and slowing of symptoms until a permanent cure can be found. Drugs for treatment of chorea, such as tetrabenazine are used with the dosages being increased in tandem with severity of symptoms (Videnovic et al., 2013). Other drugs such as ethyl-eicosapentaenoic acid (EPA) showed increased motor functions among patients with chorea. There is also inpatient care where the goal is to make the final years of the individual as comfortable as possible.
Conclusion:
In conclusion, HD represents a difficult challenge in regards to treatment and prevention. The mutation in HTT, characterized by polyglutamine expansion, leads to misfolded protein and serves to cause severe cognitive decline and motor retardation. The understanding of HD has developed immensely since its formal discovery in 1872, although there is more research to be conducted before a definitive cure can be found. Current treatments remain limited and only act to delay the symptoms. As a search for a cure continues, it is vital to take into account an approach that encompasses genetic research and clinical trials. Using model organisms, such as drosophila melanogaster (fruit flies), can easily assist research due to their fast generation time and fully functioning nervous system.
References:
Ajitkumar A, De Jesus O. Huntington Disease. 2023 Aug 23. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. PMID: 32644592.
Andhale R, Shrivastava D. Huntington’s Disease: A Clinical Review. Cureus. 2022 Aug 27;14(8):e28484. doi: 10.7759/cureus.28484. PMID: 36176885; PMCID: PMC9512951.
Burrus CJ, McKinstry SU, Kim N, Ozlu MI, Santoki AV, Fang FY, Ma A, Karadeniz YB, Worthington AK, Dragatsis I, Zeitlin S, Yin HH, Eroglu C. Striatal Projection Neurons Require Huntingtin for Synaptic Connectivity and Survival. Cell Rep. 2020 Jan 21;30(3):642-657.e6. doi: 10.1016/j.celrep.2019.12.069. PMID: 31968243; PMCID: PMC7025500.
Brinkman RR, Mezei MM, Theilmann J, Almqvist E, Hayden MR. The likelihood of being affected with Huntington disease by a particular age, for a specific CAG size. Am J Hum Genet. 1997 May;60(5):1202-10. PMID: 9150168; PMCID: PMC1712445.
Caron NS, Wright GEB, Hayden MR. Huntington Disease. 1998 Oct 23 [Updated 2020 Jun 11]. In: Adam MP, Feldman J, Mirzaa GM, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1305/
Chen M, Wolynes PG. Aggregation landscapes of Huntingtin exon 1 protein fragments and the critical repeat length for the onset of Huntington’s disease. Proc Natl Acad Sci U S A. 2017 Apr 25;114(17):4406-4411. doi: 10.1073/pnas.1702237114. Epub 2017 Apr 11. PMID: 28400517; PMCID: PMC5410817.
Genetic Modifiers of Huntington’s Disease (GeM-HD) Consortium. Electronic address: gusella@helix.mgh.harvard.edu; Genetic Modifiers of Huntington’s Disease (GeM-HD) Consortium. CAG Repeat Not Polyglutamine Length Determines Timing of Huntington’s Disease Onset. Cell. 2019 Aug 8;178(4):887-900.e14. doi: 10.1016/j.cell.2019.06.036. PMID: 31398342; PMCID: PMC6700281.
Lanska DJ. George Huntington (1850-1916) and hereditary chorea. J Hist Neurosci. 2000 Apr;9(1):76-89. doi: 10.1076/0964-704X(200004)9:1;1-2;FT076. PMID: 11232352.
Sawa A, Tomoda T, Bae BI. Mechanisms of neuronal cell death in Huntington’s disease. Cytogenet Genome Res. 2003;100(1-4):287-95. doi: 10.1159/000072864. PMID: 14526190.
Schulte J, Littleton JT. The biological function of the Huntingtin protein and its relevance to Huntington’s Disease pathology. Curr Trends Neurol. 2011 Jan 1;5:65-78. PMID: 22180703; PMCID: PMC3237673.
Sharma PK, Aram A, Polaka Y, Pandian V. Huntington’s Disease: A Report of an Interesting Case and Literature Review. Cureus. 2024 Mar 3;16(3):e55443. doi: 10.7759/cureus.55443. PMID: 38567236; PMCID: PMC10986899.
van Duijn E, Fernandes AR, Abreu D, Ware JJ, Neacy E, Sampaio C. Incidence of completed suicide and suicide attempts in a global prospective study of Huntington’s disease. BJPsych Open. 2021 Aug 31;7(5):e158. doi: 10.1192/bjo.2021.969. PMID: 34462049; PMCID: PMC8444051.
Videnovic A. Treatment of huntington disease. Curr Treat Options Neurol. 2013 Aug;15(4):424-38. doi: 10.1007/s11940-013-0219-8. PMID: 23417276; PMCID: PMC3677041.
Viguera E, Canceill D, Ehrlich SD. Replication slippage involves DNA polymerase pausing and dissociation. EMBO J. 2001 May 15;20(10):2587-95. doi: 10.1093/emboj/20.10.2587. PMID: 11350948; PMCID: PMC125466.
Huntington’s Disease is a progressive neurodegenerative disorder caused by a mutation in the huntingtin gene, which leads to an abnormal expansion of polyglutamine repeats. This genetic defect results in the misfolding and aggregation of proteins that primarily affect striatal neurons, which are crucial for motor and cognitive functions. Huntington’s Disease is characterized by genetic anticipation, where symptoms worsen over successive generations. The primary symptoms include chorea, cognitive decline, and behavioral changes, with onset typically occurring in someone’s 30s or 40s. However, younger cases can occur, starting as young as 12. The disease progresses over 15 to 18 years, significantly reducing life quality and expectancy. Although Huntington’s Disease is currently incurable, there are treatment strategies that focus on symptom management, such as using tetrabenazine for chorea and providing supportive care to improve patients’ quality of life. Diagnosis is confirmed through genetic testing to identify increased polyglutamine repeats. Understanding Huntington’s Disease’s pathophysiology, including the role of the huntingtin gene in axonal trafficking and gene transcription, is critical for developing effective treatments. Striatal neurons are particularly vulnerable due to their high energy demands and susceptibility to cytotoxic effects. Ongoing research emphasizes the need for genetic and clinical approaches to find a cure, with model organisms like Drosophila melanogaster has significantly helped in the exploration of potential therapeutic interventions. Despite significant advances since Huntington’s Disease identification in 1872, further research is essential to unravel the complexities of this devastating disorder and develop a definitive cure.