
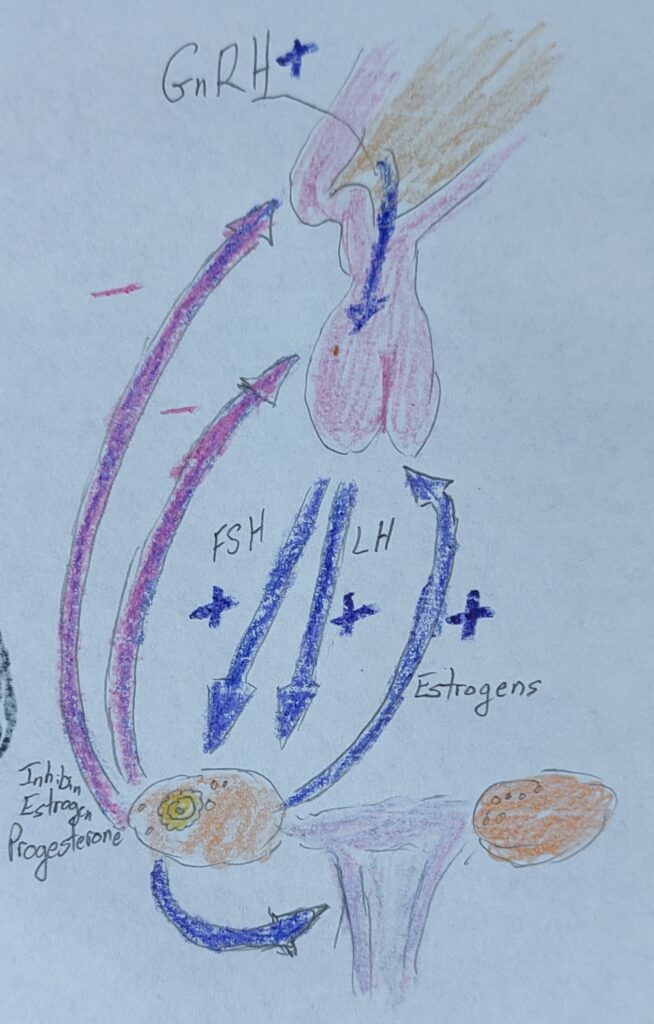
Eumenorrhea—normal menstrual/ovarian cycle: Hypothalamic pituitary ovarian axis. GnRH is secreted from the hypothalamus. Follicle-stimulating hormone (FSH) and luteinizing hormone (LH) are secreted from the anterior pituitary. FSH and LH act on theca and granulosa cells of ovarian follicles to produce estrogens (and inhibin); estrogens act on the endometrial lining to rebuild. A negative feedback loop from elevated estrogens inhibits GnRH, LH, and FSH production. All but the dominant follicle undergo atresia without FSH, continued production of estrogens from the dominant follicle results in a brief positive feedback loop and an LH surge. The LH surge results in ovulation and causes the follicle to change to the corpus luteum. The corpus luteum produces progesterone which inhibits GnRH, FSH, and LH. Without fertilization, the corpus luteum degenerates and progesterone falls, resulting in the shedding of the endometrial lining, and the cycle begins again.
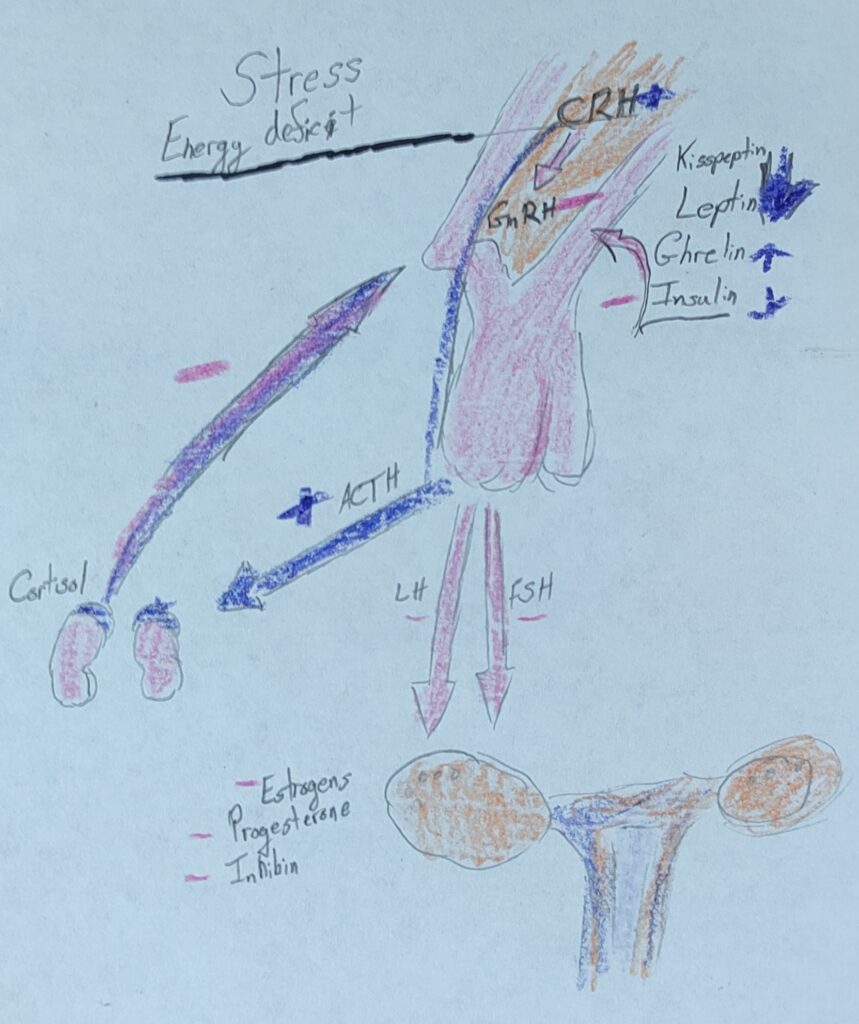
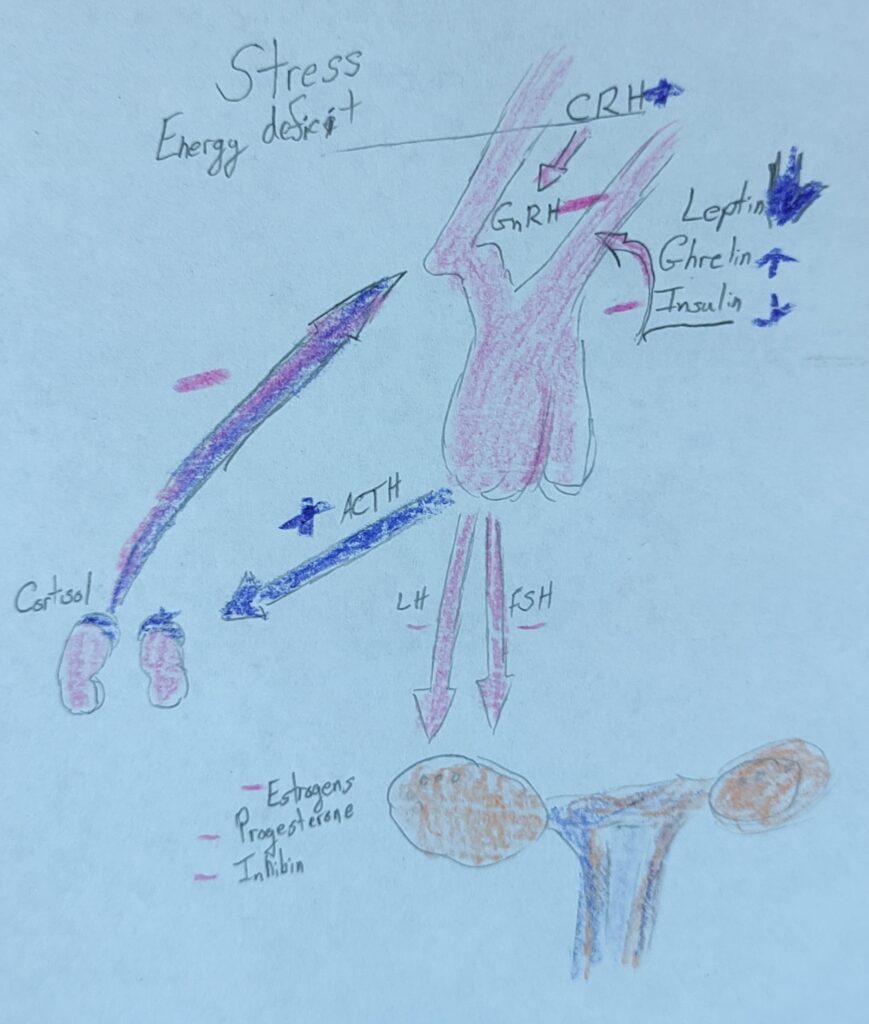
Functional hypothalamic amenorrhea: Hypothalamic pituitary adrenal (HPA) axis and HPO) axis. Normal GnRH pulsatility from the hypothalamus is inhibited by chronic activation of the HPA axis in response to stress (psychological or exercise-related), energy deficit (with or without weight loss), and related hormonal changes (e.g., increased cortisol, increased ghrelin, decreased leptin, decreased insulin, and decreased kisspeptin). The overall HPO axis is depressed, resulting in the inhibition of FSH and LH from the anterior pituitary. Ovarian follicles are not stimulated to mature, and subsequent hypoestrogenism and lower progesterone occur preventing the development, and following shedding, of the uterine lining—anovulation and a lack of menses.
Progress photos:
The STEAM-Project presented covers the functional hypothalamic amenorrhea (FHA) and how it connects to the unit 8 and unit 9 objectives. Puberty and the typical ovulatory cycles start off by the regulation on gonadotropin-releasing hormone (GnRH). In the menstrual cycle, the uterine lining will shed, rebuild, and prepare itself for implantation. Amenorrhea is the deficiency of menstrual period. Two ways amenorrhea is seen is either primary or secondary. The difference between the two is that primary is the lack of menarche by fifteen and secondary is lack of menses for three consecutive cycles. That is if they previously had their ovarian and menstrual in normal cycles. If someone has FHA, they are not likely to menstruate or ovulate. The GnRH, FSH, and LH are going to depress and not introduce normal ovarian development cycles. Due to depression of HPO axis and anovulation, the release of progesterone is not able to occur without maturation of ovarian follicles. Although sometimes, the increase in GnRH Pulsatility can result in fertility or oligomenorrhea which is the opposed to amenorrhea. These opposed cycles are known to be irregular cycles. FHA can have a wide range of consequences on both mental and physical health.
The pictures presented are two drawings that illustrate the functional hypothalamic amenorrhea. The first image shows the hypothalamic-pituitary ovarian axis signifying the normal feedback loop that is present within a typical ovarian and menstrual cycle. The second image shows the activation of the hypothalamic adrenal pituitary axis and a few hormonal changes that responded to stress, energy deficit and the interference with HPO axis.