
This STEAM project is covering the four cells that comprise bone tissue. My project is on the disease Fibrodysplasia Ossificans Progressiva (FOP). FOP is a disease that affects the ligaments, tendons, and skeletal muscles and causes heterotopic bone formation. This occurs when bone tissue begins to form in soft tissues, like skeletal muscle, and gradually limits mobility eventually leading to death. This occurs due to FOP being a progressive disease. After trauma to the soft tissues inflammation in the area begins. This then triggers a heterotopic ossification episode where the muscle tissue is replaced with new bone tissues. In my painting I chose to highlight the precursors to the disease as well as the progression of FOP into its later stages. At birth an infant with FOP may show no signs of carrying the disease as bone formation does not generally occur until after large inflammation episodes occur. There is however one main sign that an infant may have FOP. According to the journal Fibrodysplasia Ossificans Progressive: Watch the Great Toes by Mutulu Kartal FOP patients are “characterized by congenital malformation of the great toes and progressive ossification” Malformed great toes are seen at birth in all FOP patients and is generally the first sign in diagnosing the condition.
The extracellular bone formation, heterotopic ossification, is attributed to circulating osteogenic precursor cells (COP). According to the journal Circulating Osteogenic Precursor Cells by Robert Pingolo COP cells are “blood-borne cells that express a variety of osteoblastic markers and are able to form bone” (Pingolo. 2016). Osteogenic cells are mitotically active cells that when stimulated can transform into other bone forming cells, osteoblasts and osteocytes. The osteogenic cells act like a STEM cell in that they can be formed into different types of cells, but specifically bone cells. The role they play in FOP is when they are circulating in the bloodstream. In normal conditions it is believed that these COP cells are used in bone cell formation during development or post-fracture. “Circulating osteoblast-lineage cells are most abundant in patients postfracture” (Pingolo. 2016). In an individual with FOP, before new extracellular bone formation, COP cells are found in high concentrations “COP cells seed sites of injury or inflammation in response to homing signals and are involved in – heterotopic bone formation” (Pingolo. 2016).
The COP cells induce bone formation by transforming into two different bone formation cells. The first being the Osteoblasts which are extracellular matrix creating cells meaning they create the collagen to provide the framework for new bone formation then crystalize the new bone with calcium-binding proteins. Osteoblasts are very mitotically active therefore they will continue to multiply at the site of inflammation furthering the bone formation. Osteocytes are mature osteoblasts that reinforce the bone from stress or fracture as well as communicate to osteoblast and osteoclast cells for bone remodeling. Bone-lining cells are flat cells that also play a role in FOP by helping maintain the newly formed bone at the original site of inflammation, by monitoring the ECM from the outer and inner parts of the bone. Interestingly the final bone cell, osteoclasts, play a very important role as to why FOP is a progressive disease that cannot be reversed. Osteoclasts are derived from white blood cells unlike the other cells that are formed from the osteogenic cells. Osteoclasts’ function is to break down bone which makes them vital in a healthy bone system. According to the journal Periodontal ligament fibroblasts as a cell model to study osteogenesis and osteoclastogenesis in FOP by Teun de Vries “osteoclast formation was significantly lowered” in patients with FOP. This is further supported through the discovery that there is no increased “capacity of FOP-derived cells to orchestrate the formation of osteoclasts” (Vries. 2018). Together this makes individuals with FOP high risk for continued progression of their disease and bone formation.
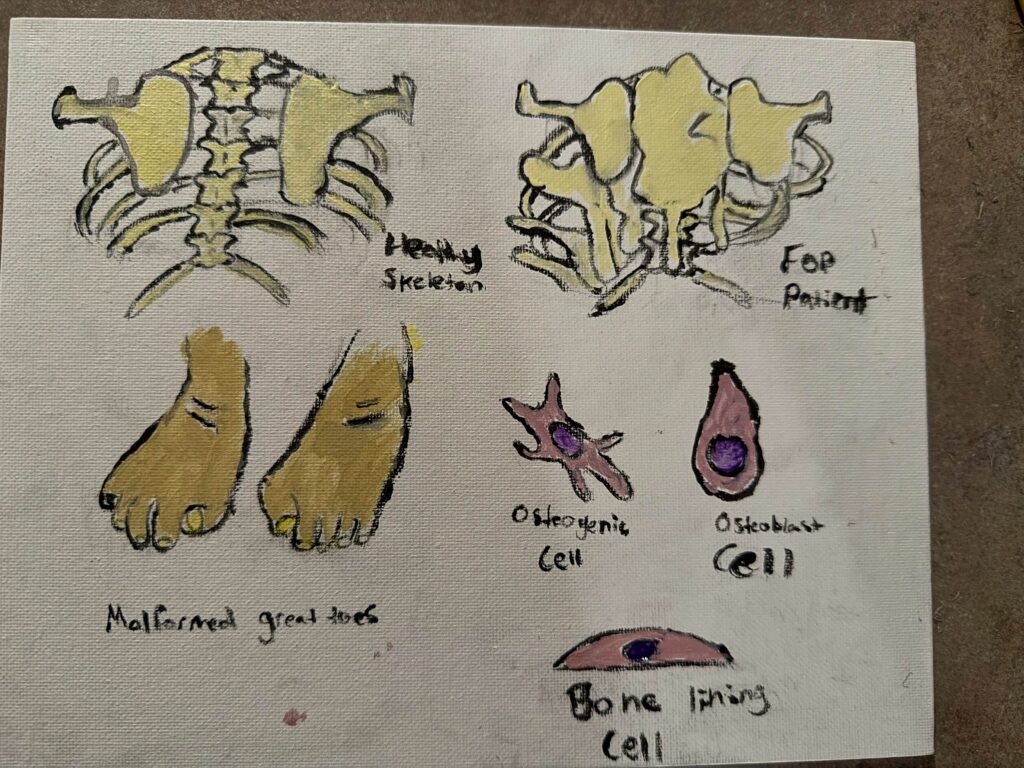
The painting I created highlights three main components of FOP. The first being the skeletal difference between a normal skeleton and the second being a skeleton with FOP. The FOP skeleton was depicted as a later stage FOP after it had progressed to a debilitating level where mobility would be limited. In the FOP skeletal painting the outer extraskeletal formation is most commonly seen in the upper back and forms a secondary outer layer. Next I chose to depict the malformed great toes as they are “present in all affected individuals” (Kartal. 2016). Lastly I created a visual representation of the osteogenic and osteoblasts cells to showcase their importance in creating the extraskeletal formation.
Works Cited
de Vries, T. J., Schoenmaker, T., Micha, D., Hogervorst, J., Bouskla, S., Forouzanfar, T., Pals, G., Netelenbos, C., Eekhoff, E. M. W., & Bravenboer, N. (2018). Periodontal ligament fibroblasts as a cell model to study osteogenesis and osteoclastogenesis in fibrodysplasia ossificans progressiva. Bone, 109, 168–177. Periodontal ligament fibroblasts as a cell model to study osteogenesis and osteoclastogenesis in fibrodysplasia ossificans progressiva – ScienceDirect
Kartal-Kaess, M., Shore, E. M., Xu, M., Schwering, L., Uhl, M., Korinthenberg, R., Niemeyer, C., Kaplan, F. S., & Lauten, M. (2010). Fibrodysplasia ossificans progressiva (FOP): watch the great toes!. European journal of pediatrics, 169(11), 1417–1421. https://doi.org/10.1007/s00431-010-1232-5
Pignolo RJ, Shore EM. Circulating osteogenic precursor cells. Crit Rev Eukaryot Gene Expr. 2010;20(2):171-80. doi: 10.1615/critreveukargeneexpr.v20.i2.70. PMID: 21133846; PMCID: PMC3753686.https://pmc.ncbi.nlm.nih.gov/articles/PMC3753686/#:~:text=Circulating%20osteogenic%20precursor%20(COP)%20cells,and%20are%20of%20hematopoietic%20origin.
Fibrodysplasia Ossificans Progressiva (FOP) is an inheritable and progressive disease that results in excess bone growth in soft tissue areas. This ties into our in class objective: Identify the 4 cells that comprise bone tissue. FOP occurs as osteogenic precursor cells (COP), cells that circulate in the bloodstream and are related to bone cell formation, transform into excessive amounts of osteoblasts and osteocytes. This is triggered by trauma to a soft tissue, resulting in FOP and subsequent ossification of the muscle tissue. Together osteoblasts, which function to lay down collagen (the groundwork for bone structure), and osteocytes, which reinforce bone due to stress or fracture in normal conditions, work to form new bone in those with the disease. Bone lining cells then function to maintain this new bone. And lastly osteoclasts, which are cells responsible for breaking down bone, are unfortunately found in much lower numbers in persons with this disease. This all together results in the excessive bone formation and maintenance and few osteoclasts to break down unwanted bone. Given time this progressive disease cannot be reversed and actually gets worse. Persons suffering from FOP can experience drastically decreased mobility and life-limiting as a result.