This work is meant to Identify the effect of cachexia/Hypermetabolism on the Skeletal Muscle and bone tissues in response to burning wounds. It is also meant to identify the aforementioned tissues and their functions.
Victims who suffer burns from stage 4 and up face a lot of issues when beginning the healing process. Along with the lymphatic system, respiratory system, and nervous system, major tissues that are badly affected are the Skeletal and muscle tissues. Both of these are fairly regenerative tissues but muscle tissue more so, and while they do undergo a healing process, they are not the same on a cellular level after being damaged by burns. These two tissues are the focus of burn induced cachexia and hypermetabolism, which cause dysfunction in muscle and bone tissues.
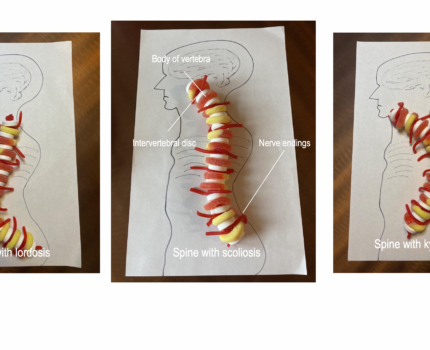
Bones(Osseous tissue) are present throughout the body, supporting other tissues. When burned in an accident they can face a multitude of issues, the first of which being bone loss or loss of bone mineral content(BMC). This burn injury results in a rise of proinflammatory cytokines which are as the name states “Proinflammatory” and do not promote healing. Through a chain of cellular interactions, these cytokines stimulate osteoclast activity. Therefore hastening bone resorption into the bloodstream. Other factors also play a role in the stimulation of osteoclast activity, and inhibition of osteoblasts. This means that bone resorption or degradation is increased while bone production is lowered.
It is also notable that Parathyroid hormone(PTH) is much lower than what is required to regulate the calcium and phosphorus in the body in burn victims. Thus the calcium metabolism is no longer in good condition to regulate our calcium levels in a productive way.
Our Skeletal muscle is all over the body with origins and insertions along our bones. These tissues are in charge of voluntary movement, locomotion, and environmental manipulation. These contractile tissues are adversely affected by burns, and the key term to understanding burn induced muscle cachexia is hypermetabolism. Hypermetabolism is an increase in resting metabolic activity, in this case in response to the burn wound. The now hyperactive metabolism sets off an increase of stress regulators, such as catecholamines and glucocorticoids. These induce hypercatabolic responses, particularly proteolysis, which is the breakdown of proteins and peptides. This breakdown of proteins in the muscle, as well as other miscellaneous tissues within the body, become the fuel source for the hyperactive metabolism, and are used to heal the wound.
This degradation of tissues due to a disturbed calcium metabolism, and a hyperactive metabolism weakens the body in order to heal burn wounds, and continues to be catabolic after the wound has healed, even continuing three years after the injury takes place. This is costly to the body and can actually bring harm to the body in the form of sepsis, organ failure, early stages of osteoporosis, and other medical complications.
Burns and wounds. Burns and Wounds | Johns Hopkins Medicine. (n.d.). Retrieved November 8, 2022, from https://www.hopkinsmedicine.org/health/conditions-and-diseases/burns#:~:text=Second%2Ddegree%20burns%20involve%20the,may%20be%20swollen%20and%20painful.&text=Third%2Ddegree%20burns%20destroy%20the,bones%2C%20muscles%2C%20and%20tendons
Cherney, K. (2019, June 4). 4th degree burn and other degrees: Classification, healing, more. Healthline. Retrieved November 8, 2022, from https://www.healthline.com/health/4th-degree-burn
Klein, G. L. (2006, August 8). Burn-induced bone loss: Importance, mechanisms, and management. Journal of burns and wounds. Retrieved November 8, 2022, from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1687146/
Knuth, Carly M, et al. “Burn-Induced Hypermetabolism and Skeletal Muscle Dysfunction.” American Journal of Physiology. Cell Physiology, U.S. National Library of Medicine, 1 July 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8321793/
CA;, Dinarello. “Proinflammatory Cytokines.” Chest, U.S. National Library of Medicine, Aug. 2000, https://pubmed.ncbi.nlm.nih.gov/10936147/
One Comment